(Urotoday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Siamak Daneshmand, MD, discussing a matching adjusted indirect comparison of TAR-200 versus FDA-approved novel agents in BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS. TAR-200 is a novel intravesical drug-releasing system designed for sustained, local delivery of gemcitabine within the bladder. TAR-200 is being investigated in the phase 2b SunRISe-1 study for patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS, with or without papillary tumors, who have refused or are ineligible for radical cystectomy (Cohort 2)1. Moreover, TAR-200 has demonstrated a centrally assessed any time complete response rate of 82.4% in this population. Previously, the FDA has approved pembrolizumab2, nadofaragene firadenovec-vncg (nadofaragene)3, and nogapendekin alfa inbakicept-pmln (NAI) + BCG4 for the treatment of patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS. In the absence of head-to-head data, matching adjusted indirect comparisons were conducted to compare complete response of TAR-200 versus FDA-approved novel agents.
A systematic literature review identified published data on the comparator regimens in the BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS setting. The feasibility of conducting matching-adjusted indirect comparisons was assessed by reviewing the study and patient characteristics, patient eligibility criteria, outcome definitions, and time points of SunRISe-1 and trials of FDA-approved novel agents —KEYNOTE-057, CS-003, and QUILT 3.032 — to determine heterogeneity. Three unanchored matching adjusted indirect comparisons were conducted using individual patient data from SunRISe-1 Cohort 2 and summary-level data from the US prescribing information and primary journal publications of the comparators. Imbalances in patient characteristics (tumor stage, prior doses of BCG instillation, ECOG performance status, age, gender, and race) were adjusted by weighting the TAR-200 individual patient data to match the reported baseline characteristics of the comparator trials. Comparative efficacy was estimated for complete response rate at any time and at first disease assessment. Relative effects were quantified using rate differences with 95% confidence intervals derived from weighted logistic regression analysis.
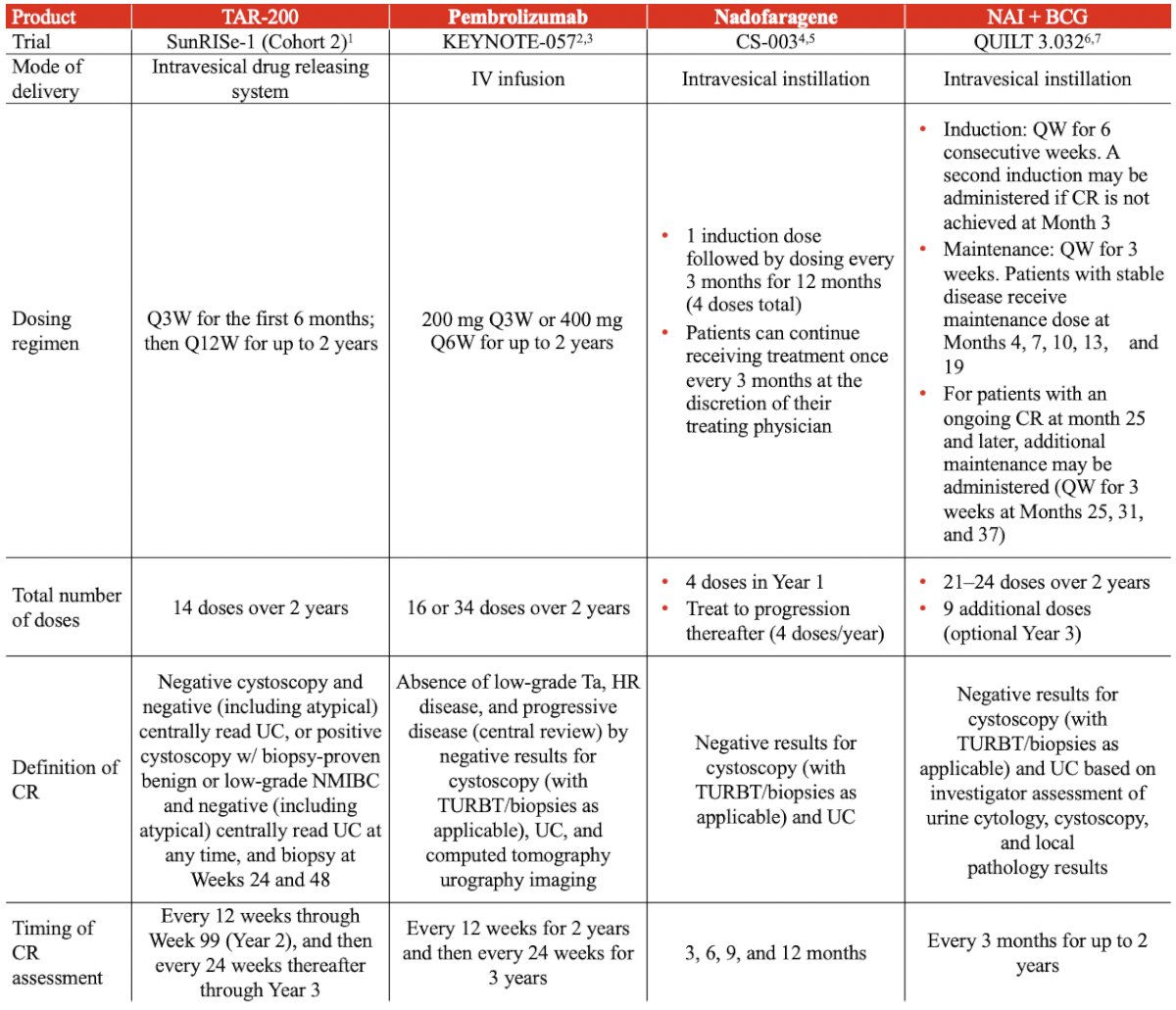
Dosing regimens, modes of delivery, and definitions of complete response varied across the SunRISe-1, KEYNOTE-057, CS-003, and QUILT 3.032 trials:
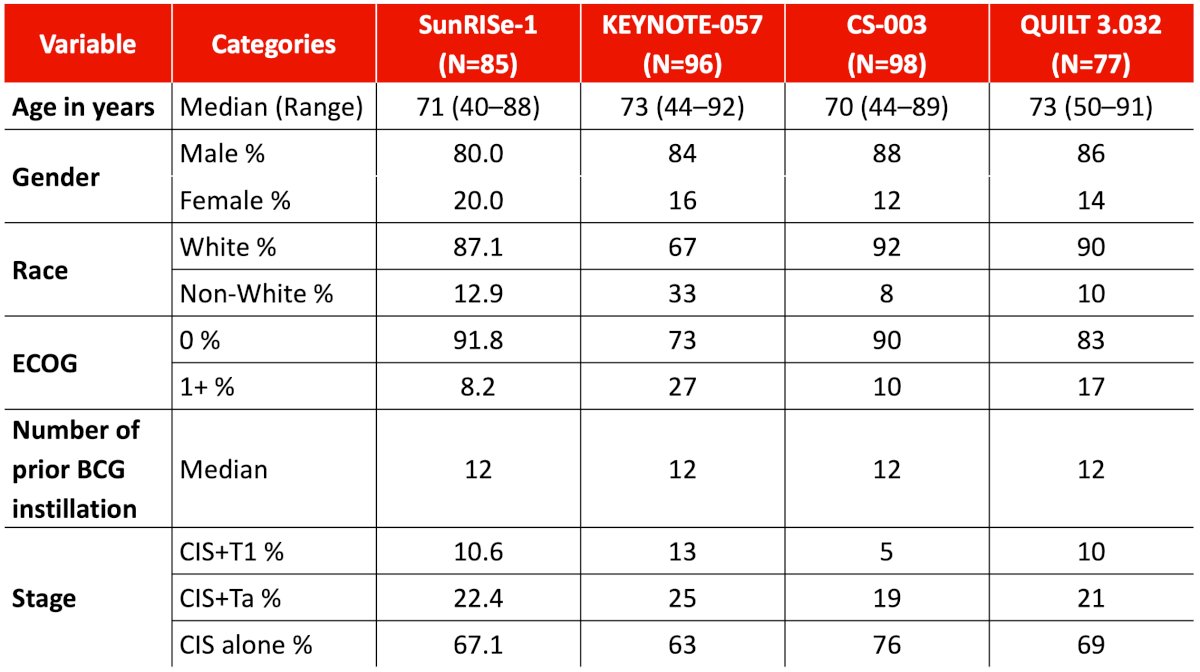
Baseline characteristics were similar across all four trials after matching:
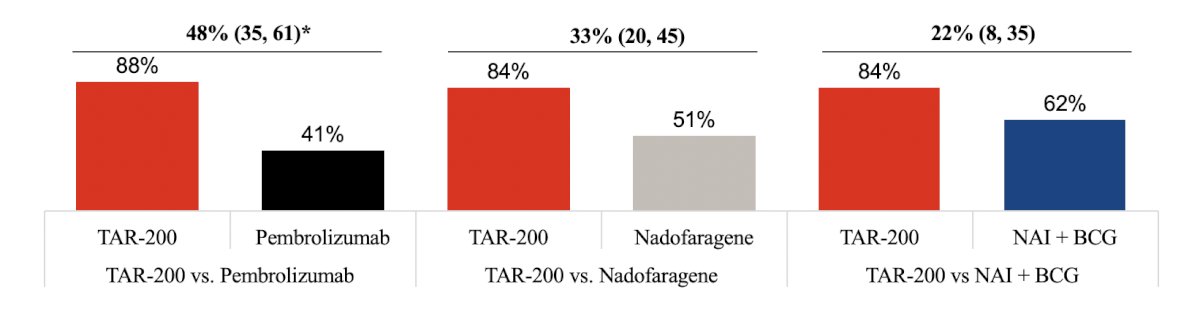
After adjustment, the three matching adjusted indirect comparisons showed that TAR-200 provides significantly higher complete response rate at any time versus all three FDA-approved novel agents (p < 0.05 for all comparisons) in the BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS setting. The greatest incremental difference was observed in the TAR-200 versus pembrolizumab comparison (+48%):
Given that re-induction was allowed in QUILT 3.032, an analysis comparing complete response rate at first disease assessment of TAR-200 versus NAI + BCG was conducted to assess the impact of re-induction on complete response rate:
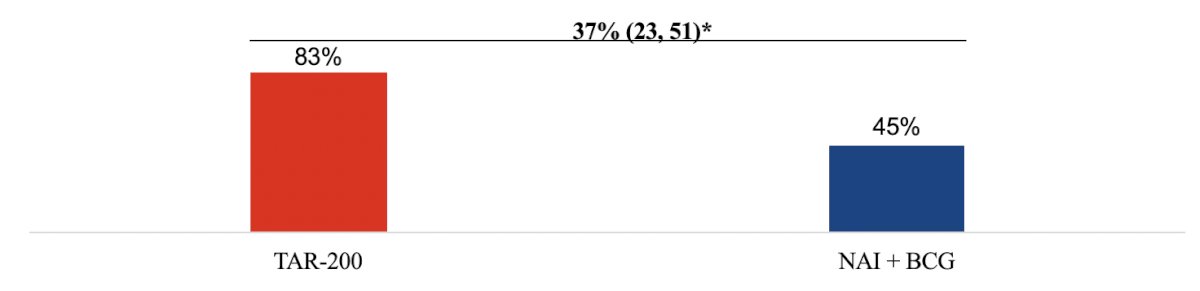
Results from this analysis showed that treatment with TAR-200 led to a significantly higher complete response rate at first disease assessment compared with NAI + BCG (p < 0.05) based on calculated data that excluded patients who received a second induction.
Additional details for the calculation of complete response at first disease assessment for NAI + BCG are as follows:
- In the US prescribing information, the efficacy results from QUILT 3.032 (n = 77) state that 62% achieved complete response at any time (n = 48 responders). The US prescribing information also states that 31% (n = 24) of patients received a second induction course
- Chamie et al.4 also state that 24 patients received re-induction in Cohort A
- Thus, the investigators deduced that the 24 re-induced patients are the same across both data sets. Chamie et al.4 state that of the 24 re-induced patients, 13 achieved complete response after re-induction
- Triangulating between the sources, Dr. Daneshmand and colleagues calculated from the US prescribing information that 48 total responders – 13 responders after re-induction/77 total patients = 45% of patients achieving complete response at first disease assessment
Limitations of this analysis include the matching adjusted indirect comparison methodology only adjusting for observed and reported baseline characteristics. Additionally, any confounders not consistently reported or missing across studies may impact internal validity. Finally, some differences in study design and outcomes can introduce biases that the matching-adjusted indirect comparison cannot fully address.
Dr. Daneshmand concluded his presentation discussing a matching-adjusted indirect comparison of TAR-200 versus FDA-approved novel agents in BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS, and included the following take-home points:
- TAR-200 is a novel intravesical drug release system that offers a convenient fixed duration treatment regimen with a low number of doses for patients with BCG unresponsive high-risk non-muscle invasive bladder cancer with CIS, without the need for re-induction
- Given that no head-to-head trials exist in this setting, the matching adjusted indirect comparison provides scientific information for clinical and reimbursement decision-making making
- TAR-200 provides a statistically significant clinical benefit in complete response rate at any time versus pembrolizumab, nadofaragene, and NAI + BCG
- TAR-200 also provides a significantly higher complete response rate at first disease assessment compared with NAI + BCG
Presented by: Siamak Daneshmand, University of Southern California, Norris Comprehensive Cancer Center, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.
References:
- Daneshmand S, Van der Heijden MS, Jacob JM, et al. TAR-200 for Bacillus Calmette-Guerin-Unresponsive High-Risk Non-Muscle-Invasive Bladder Cancer: Results from the Phase IIb SunRISe-1 Study. J Clin Oncol. 2025 Jul 30 [Epub ahead of print].
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021 Jan;22(1):107-117.
- Chamie K, Chang SS, Kramolowsky E, et al. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022; 2(1).