(UroToday.com) During the WCET Basic Science Poster Session, Dr. David Lifshitz started his presentation by bringing to attention the lack of extensive research studying the impact of decreased urinary uric acid (UA) concentration on UA stone dissolution that has led to inconsistent treatment guidelines.
Currently, there is a guideline discrepancy such that the European Association of Urology promotes the use of allopurinol, a medication to prevent and reduce UA formation, for hyperuricosuria, while the American Urological Association indicates its use only when urine alkalinization is insufficient in reducing uric acid stones. To improve our understanding and clarify this discrepancy, Dr. Lifshitz investigates the in vitro effect of lower urinary UA concentration on UA stone dissolution as well as the role of alkalinization in modulating this effect.
Dr. Lifshitz and his team utilized X-ray diffraction to analyze and verify UA stones obtained from patients who had undergone percutaneous nephrolithotomy. Urine spot tests were performed on healthy volunteers who had no stones to establish a mean urine UA saturation level. UV-Vis spectrophotometry was used to assess UA dissolution kinetics of undersaturated UA solutions of increasing concentration increments in an artificial urine solution setup at 37°C at pH values of 5.5, 6, 6.5, 7, and 7.2 (Figure 1).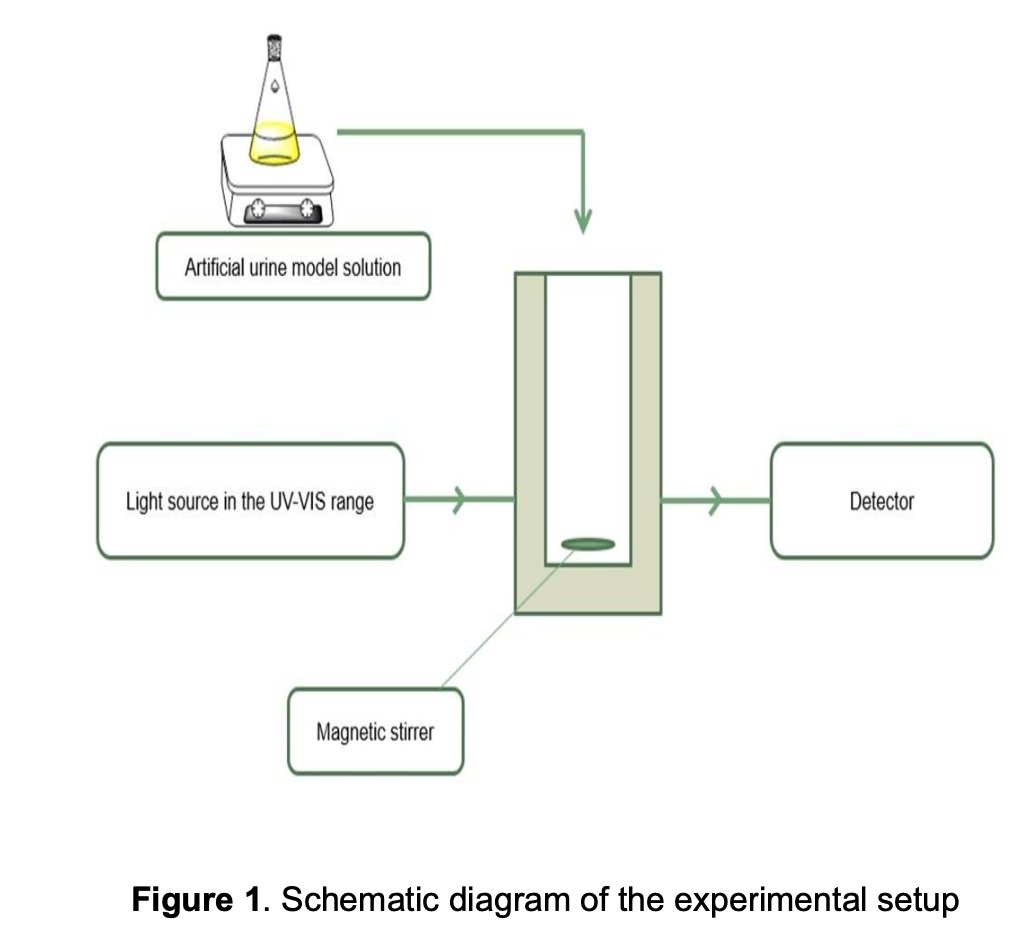
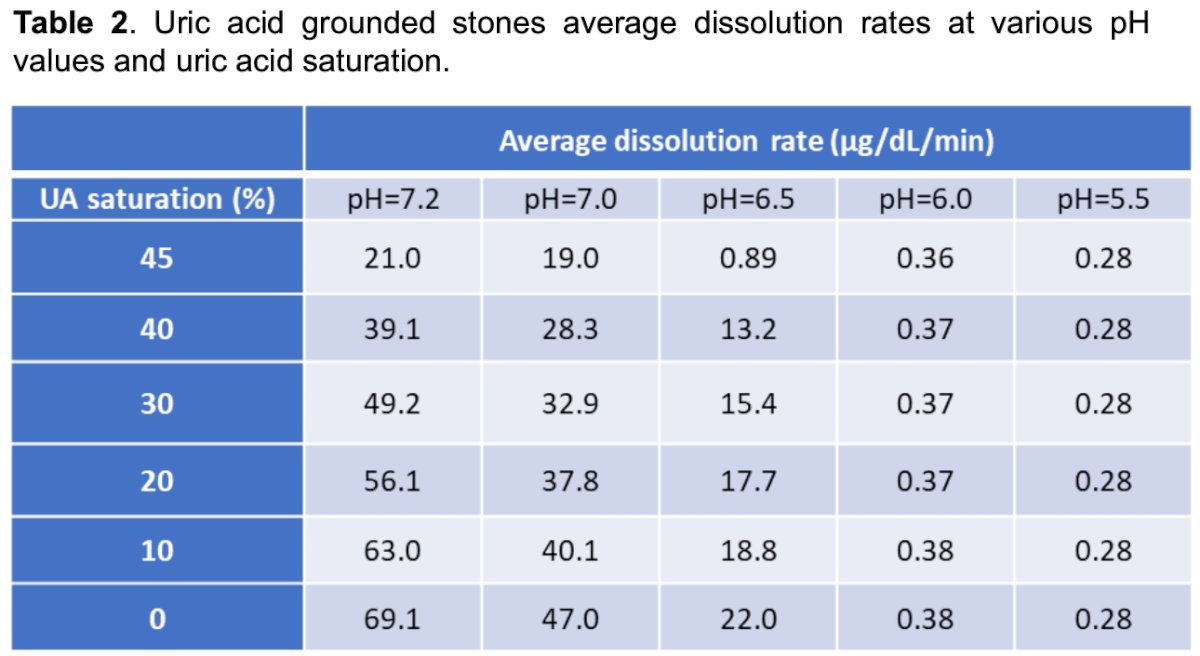
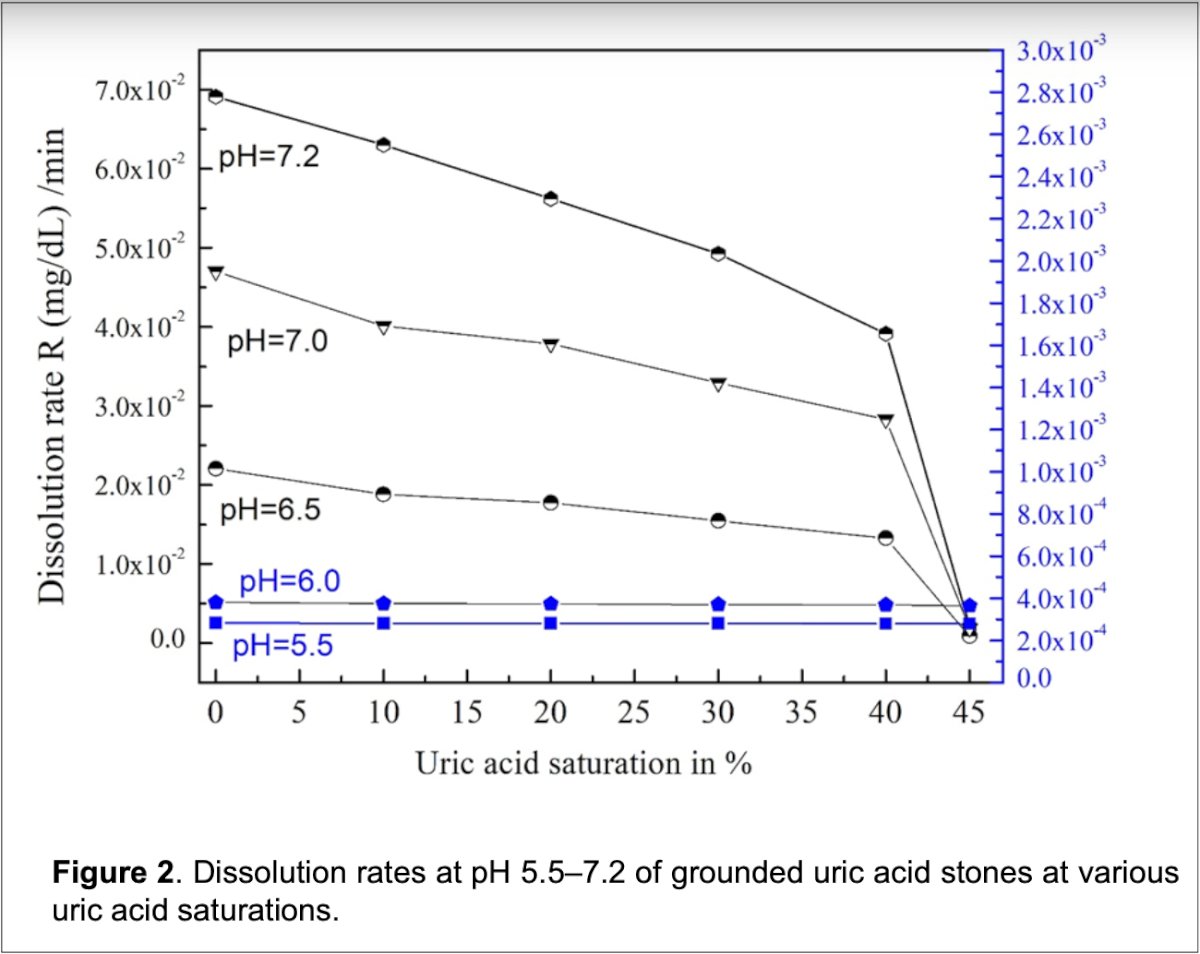
Their work determined the normal UA saturation concentration to be 29.4 mg/dL. Additionally, Dr. Lifshitz highlights the finding that lowering urine UA levels only increased UA dissolution at pH > 6.5 and after reducing UA concentration to 55% of the normal level. Furthermore, the highest increase in dissolution rate was found to occur at pH = 7.2 when UA concentration is between 45% and 30% of the normal level (Table 2 and Figure 2).
Dr. Lifshitz concluded his presentation with the main takeaway that adequate alkalinization (pH > 6.5) is a key step needed to dissolve UA stones which can then be further dissolved with a reduction in UA levels.
The Q&A portion started with a question from Dr. Ralph Clayman from the audience, who asked: For patients who come to you with a CT showing 400 HU and a urine pH of 5, would you treat them with alkalinization or operate on them? Dr. Lifshitz replies that he would start off with an alkalinization trial. Dr. Clayman followed up, asking Dr. Lifshitz what approach he would take to alkalinize the urine, to which he responded that he would provide Urocit-K if the patient’s GFR was normal and adjust accordingly. Dr. Lifshitz closes with the statement that the main issue at hand is picking the appropriate patient, which is difficult, as many patients have uric acid stones that are impure.
Presented by: David Lifshitz, Professor and Managing Director of Endourology, Rabin Medical Center, Petah Tiqwa, Israel
Written by: Victor Pham, BS, University of California, Irvine, @victorpham01 on X during the 2025 World Congress of Endourology and Uro-Technology (WCET) Annual Meeting: September 8 – September 12, 2025, Phoenix, Arizona