(UroToday.com) The 2025 SUO Annual Meeting featured a poster by Dr. Girish S. Kulkarni and colleagues reporting real-world outcomes for patients with high-risk non-muscle invasive bladder cancer (HR-NMIBC) with carcinoma in situ (CIS) who became BCG-unresponsive and subsequently received intravesical chemotherapy. For HR-NMIBC, BCG remains the standard of care,1 yet up to 40% of patients ultimately become unresponsive, at which point they face substantially increased risks of disease recurrence and progression.2,3 Although radical cystectomy is guideline-recommended for BCG-unresponsive CIS, real-world uptake remains low due to procedural morbidity and quality-of-life considerations. In the U.S., IVES chemotherapy has become the most commonly used salvage approach.4
Because treatment response and recurrence outcomes are often unavailable in structured data sources such as payer claims and electronic medical records, this analysis leveraged clinical notes from the AQUA Registry—linked to Komodo Health claims—to capture real-world response, duration, and event-free survival for IVES chemo. The study objective was to characterize real-world outcomes—including complete response (CR), duration of response (DoR), and event-free survival (EFS)—in patients with BCG-unresponsive HR-NMIBC with CIS treated with intravesical chemotherapy.
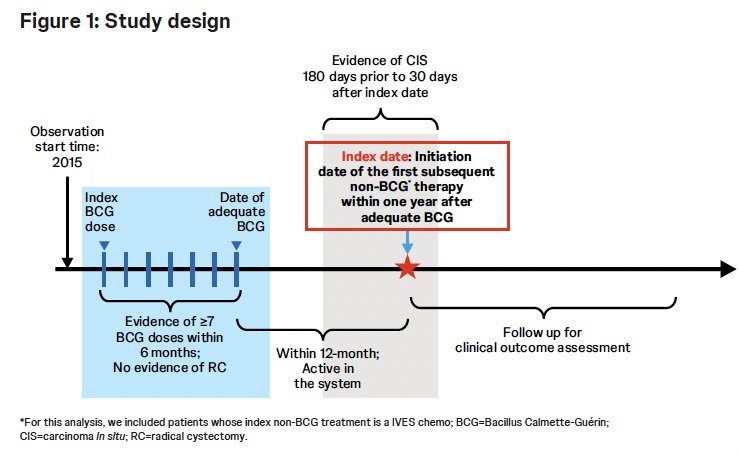
The study analyzed patient charts and electronic medical records from the American Urological Association Quality (AQUA) Registry’s NMIBC module, linked with Komodo Health claims. Adult patients were included if they:
- Had BCG-unresponsive HR-NMIBC with CIS
- Initiated intravesical chemotherapy between 2015 and 2022
- Received adequate BCG (≥7 doses within 6 months) and began non-BCG therapy within 1 year of completing adequate BCG
- Had documented CIS/TIS within 180 days before and 30 days after the index date
- Had ≥1 all-cause medical record during the 12-month post-index period
The study definitions were as follows:
- Complete response (CR): Negative cystoscopy, negative cytology or pathology, or physician documentation from unstructured notes.
- Duration of response (DoR): Time from first CR to earliest high-risk recurrence, treatment change, progression to ≥T2 or metastatic disease, or death.
- Event-free survival (EFS): Time from intravesical chemotherapy initiation to persistent disease at first assessment, high-risk recurrence, progression, subsequent therapy after cystoscopy/TURBT/biopsy, or death.
The outcomes assessed were:
- CR rate
- DoR among responders
- EFS among all treated patients
- Baseline characteristics, intravesical chemotherapy patterns
A total of 134 patients with BCG-unresponsive HR-NMIBC with CIS initiated intravesical chemotherapy. The key demographics were as follows:
- Median age: 75 years (range 55–88)
- Male: 82.1%
- White race: 91.3%
- Tumor stage: CIS only 67.2%; CIS + papillary 32.8%
- Median prior BCG doses: 12 (range 7–19)
The most used intravesical chemotherapy agents were:
- Mitomycin: 36.6%
- Gemcitabine: 29.9%
- Others: valrubicin, gemcitabine/docetaxel
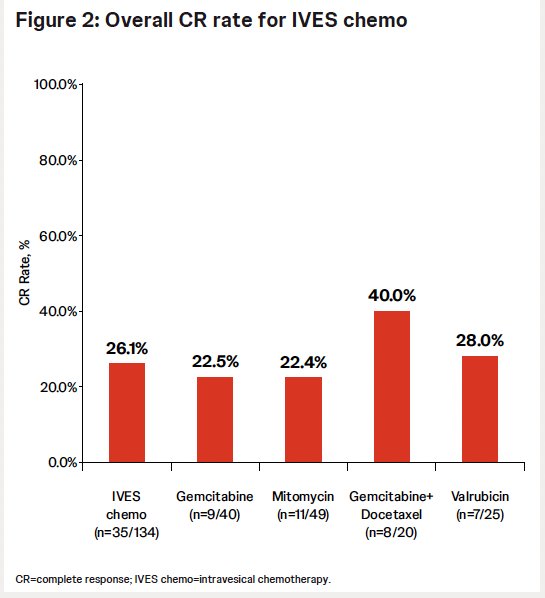
Among all intravesical therapy-treated patients, the CR rates were as follows:
- Gemcitabine: 22.5% (9/40)
- Mitomycin: 22.4% (11/49)
- Valrubicin: 28% (7/25)
- Gemcitabine/docetaxel: 40% (8/20)
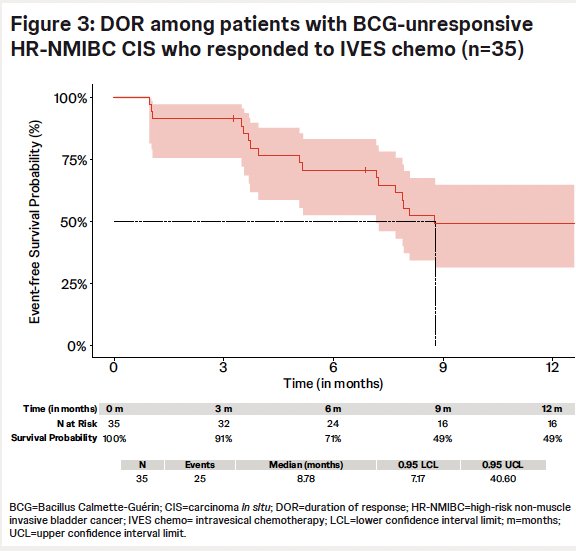
Among responders, the median DoR was 8.8 months. By 9 months, 51% of responders experienced high-risk recurrence, treatment change, progression, or death
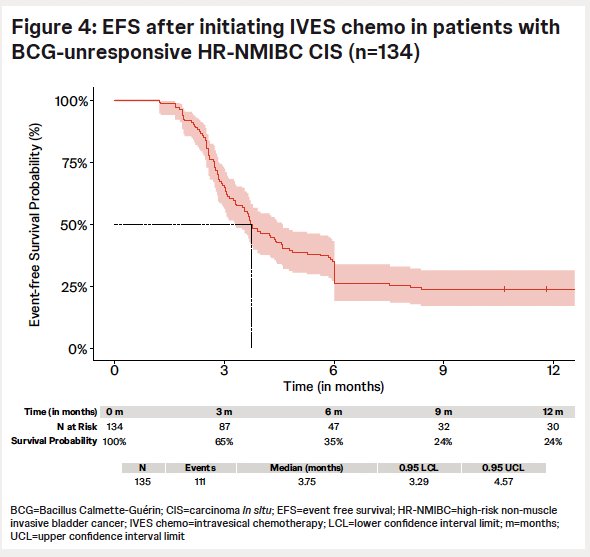
Among all patients treated with intravesical chemotherapy, the median EFS was 3.8 months. By 9 months, 76% of participants had experienced an EFS event.
The study is limited by its small sample size, retrospective design, absence of central pathology review, and incomplete clinical data inherent to registry sources. AQUA primarily captures community urology practices; therefore, non-urological comorbidities and events in other care settings may be under-represented. Additionally, participation in AQUA is voluntary and may not reflect the full diversity of U.S. urologic practice.
Dr. Kulkarni concluded that despite being the most commonly used salvage therapy for BCG-unresponsive HR-NMIBC with CIS in the U.S., intravesical chemotherapy demonstrated suboptimal real-world effectiveness, with:
- Only a small proportion of patients achieve CR
- Median DoR of 8.8 months among responders
- Median EFS of just 3.75 months, with most patients experiencing persistent disease, recurrence, progression, or death within a short timeframe
These findings underscore a substantial unmet need for more effective, durable, and innovative bladder-sparing treatment options for BCG-unresponsive HR-NMIBC with CIS.
Presented by: Girish Kulkarni, MD, PhD, Professor, Department of Surgery, Division of Urology, University of Toronto, Toronto, ON, Canada
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References:
- Holzbeierlein JM, Meng MV, Chang SS, et al. Diagnosis and treatment of non-muscle invasive bladder cancer. J Urol. 2024; 211(4):533-538.
- Lightfoot AJ, Breyer BN, Rosevear HM, et al. Management of BCG-unresponsive bladder cancer. ScientificWorldJournal. 2011; 11:602-613.
- Chang SS, Boorjian SA, Chou R, et al. AUA/SUO guideline: Diagnosis and treatment of NMIBC. 2020.
- Williams SB, McGregor B, Kamat AM, et al. Real-world management patterns in BCG-unresponsive NMIBC. Presented at AUA 2025; Las Vegas, NV.