(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a prostate cancer poster session. Dr. Charmi Patel presented the results of a real-world assessment of new-onset central nervous system (CNS) conditions in patients with non-metastatic castration-resistant prostate cancer (nmCRPC) treated with apalutamide, darolutamide, or enzalutamide.
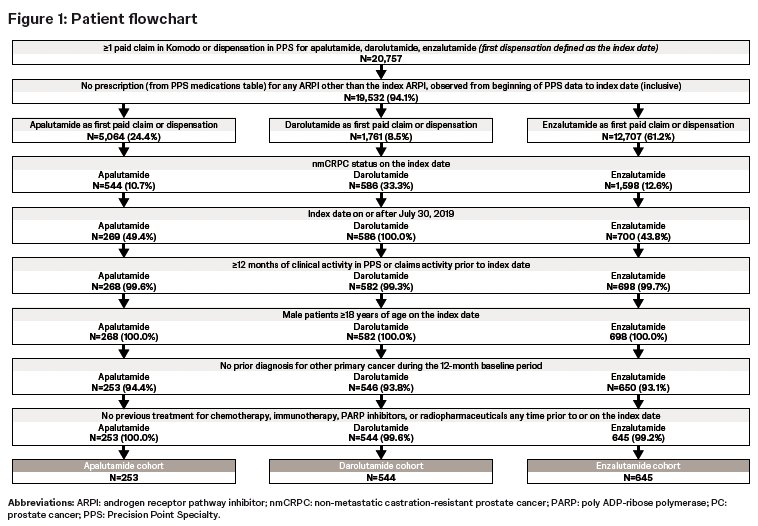
Apalutamide, darolutamide, and enzalutamide are all FDA-approved androgen receptor pathway inhibitors (ARPIs) for nmCRPC.1–3 CNS effects—including cognitive impairment, fatigue, dizziness, falls, seizures, and headaches—are clinically meaningful concerns in this population due to both baseline vulnerabilities and potential treatment-related toxicities.4–5 Despite widespread ARPI use, comparative real-world data on CNS outcomes remain limited.6 This study leveraged a large linked EMR-claims dataset to compare the incidence and timing of new-onset CNS events following ARPI initiation.This retrospective, observational study used EMR data from Precision Point Specialty (PPS) Analytics linked to Komodo Research Database claims (study period: January 1, 2016–August 31, 2024). Patients were assigned to mutually exclusive cohorts based on the first dispensation or paid pharmacy claim for apalutamide, darolutamide, or enzalutamide.
The index date was the first ARPI claim on or after July 30, 2019—the FDA approval date for darolutamide, which followed the approvals of apalutamide and enzalutamide.1–3 Patients required ≥12 months of PPS clinical activity or claims activity before the index date. ADT use was not required for cohort entry. The observation period spanned from index date until ARPI discontinuation/switch, initiation of later-line advanced prostate cancer therapy, or end of data availability.
CNS-related conditions included amnesia, anxiety, ataxia, cognitive disorders, confusion, depression, dizziness, insomnia, fatigue/asthenia, headaches, falls, pain, paresthesia, psychosis, seizures, vertigo, weakness, and other neurologic symptoms. Only new-onset events absent during the 12-month baseline period were counted.
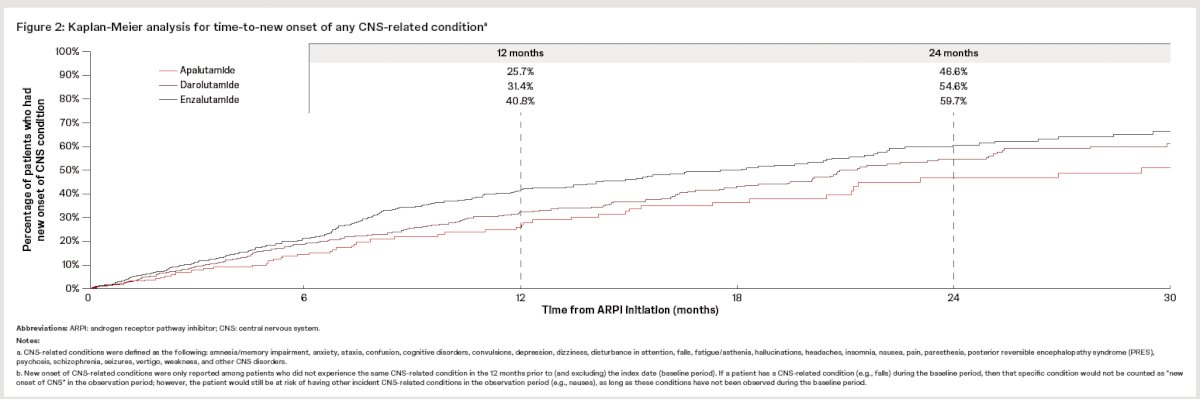
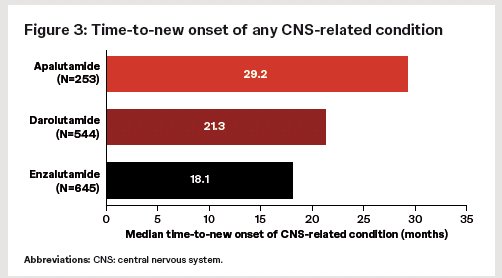
The study outcomes were the 12- and 24-month cumulative incidence rates of new-onset CNS events and median time-to-event, estimated using Kaplan-Meier methods. Analyses were descriptive.
A total of 1,442 men with nmCRPC met the study eligibility criteria:
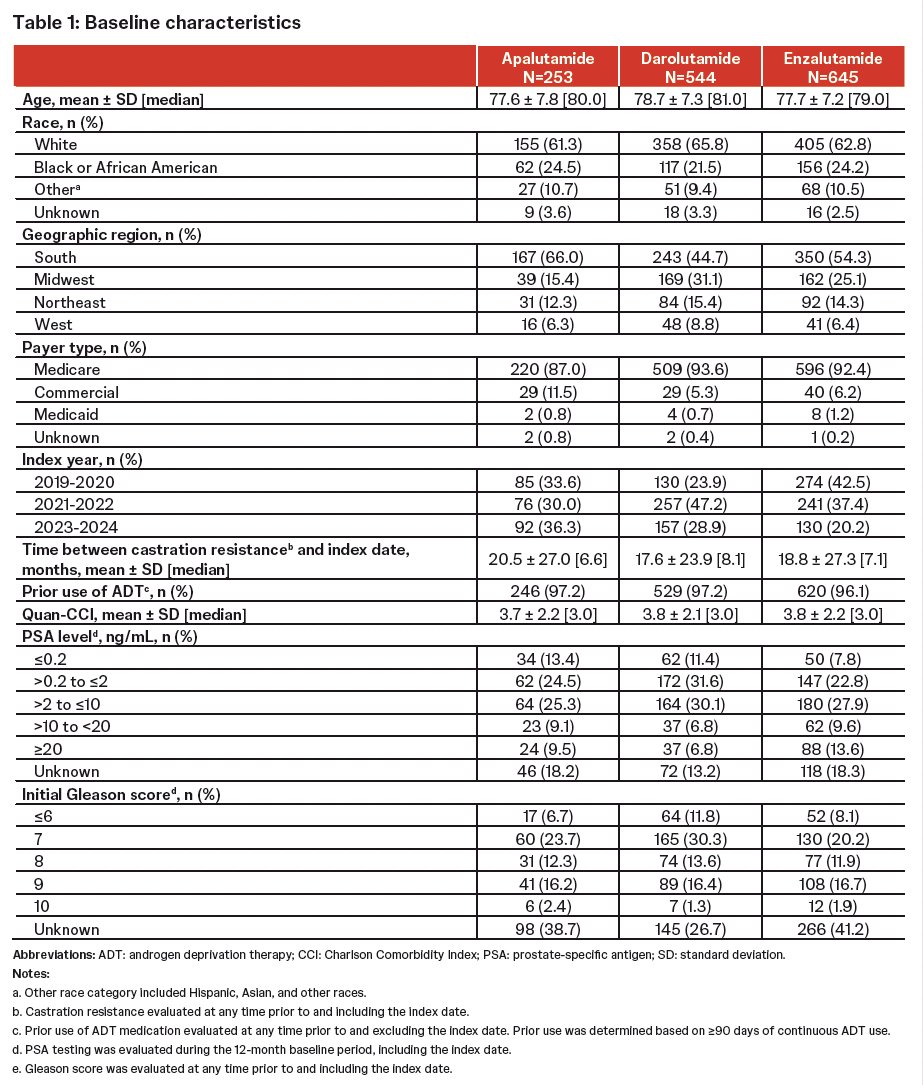
The baseline characteristics were as follows:
- Apalutamide: n = 253
- Mean age 77.6 years; 61.3% White, 24.5% Black; 87% Medicare; 97.2% prior ADT
- Darolutamide: n = 544
- Mean age 78.7; 65.8% White, 21.5% Black; 93.6% Medicare; 97.2% prior ADT
- Enzalutamide: n = 645
- Mean age 77.7; 62.8% White, 24.2% Black; 92.4% Medicare; 96.1% prior ADT
The median PSA at baseline was similar across groups, with approximately one-third in each cohort having serum PSA levels of 2–10 ng/mL. The median time from castration resistance to index date ranged from 6.6–8.1 months.
The mean (median) on-treatment observation time was as follows:
- Apalutamide: 12.4 (7.4) months
- Darolutamide: 14 (9.3) months
- Enzalutamide: 12.3 (7.7) months
The new-onset rates for commonly observed CNS effects were as follows:
Apalutamide (n=253):
- Fatigue: 7.5%
- Falls: 6.7%
- Pain: 5.1%
- Dizziness: 5.1%
- Weakness: 3.6%
- Headache: 3.2%
Darolutamide (n=544):
- Fatigue: 7.9%
- Falls: 10.3%
- Dizziness: 6.1%
- Pain: 5.7%
- Weakness: 5.3%
Enzalutamide (n=645):
- Fatigue: 9.6%
- Dizziness: 5.1%
- Pain: 9.1%
- Falls: 5.1%
- Weakness: 6.7%
Across all categories, apalutamide consistently demonstrated the lowest or near-lowest rates of new-onset CNS effects, with enzalutamide demonstrating the highest rates for many events.

With regards to potential study limitations, this study was retrospective in nature and used EMR-linked claims data, which may include coding inaccuracies and incomplete capture data. Potential mis-linkage between PPS and Komodo data remains possible. CNS symptoms may have been under-recognized, and causality cannot be established.
Dr. Patel concluded as follows:
- In this large US real-world analysis, apalutamide was associated with the lowest cumulative incidence and the longest time-to-onset of CNS-related events among ARPIs used for nmCRPC.
- Darolutamide showed intermediate rates, while enzalutamide demonstrated the highest incidence and earliest onset.
- These findings suggest clinically meaningful differences in CNS tolerability among ARPIs and may inform personalized treatment selection for patients at higher risk of neurologic toxicity.
- Continued long-term follow-up and additional real-world analyses are needed to further define CNS safety profiles across ARPI options.
Presented by: Charmi Patel, MD, St. Mary's Heathcare System
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.References:
- U.S. Food and Drug Administration. FDA approves apalutamide for non-metastatic castration-resistant prostate cancer. 2018.
- U.S. Food and Drug Administration. FDA approves darolutamide for non-metastatic castration-resistant prostate cancer. 2019.
- U.S. Food and Drug Administration. FDA approves enzalutamide for castration-resistant prostate cancer. 2018.
- Bubendorf L, Schöpfer A, Wagner U, et al. Metastatic patterns of prostate cancer: an autopsy study of 1,589 patients. Hum Pathol. 2000;31(5).
- Markman M. Managing treatment-related fatigue in patients with cancer. Clevel Clin J Med. 1999;66(10):629–631.
- Pilon D, Chow W, Ding Y, et al. Real-world management patterns of prostate cancer in the United States. Am Health Drug Benefits. 2017;10(3):143–151.