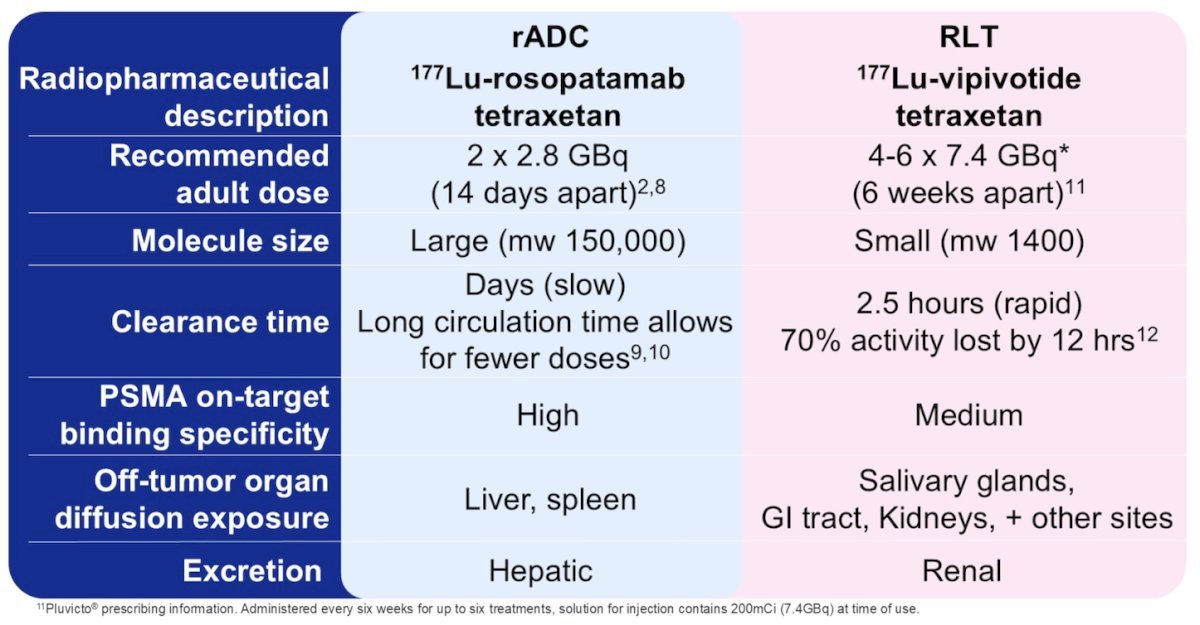
(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a prostate cancer poster session. Denise Guibault presented ProstACT Global, a phase III study of 177Lu-rosptamab + standard of care versus standard of care alone in patients with metastatic castration-resistant prostate cancer (mCRPC). The treatment of advanced prostate cancer is challenging, with undesirable side effects that impact patient quality of life. Radioimmunotherapy can localize therapy to specific tumor cells in multiple organs to reduce or eliminate damage to normal tissue. The cell surface glycoprotein PSMA is an ideal therapeutic target as it is highly expressed by malignant prostate cells. There is a strong rationale for further investigation of the 177Lu-labeled, chelator-conjugated antibody, 177Lu-rosopatamab, as a potential first-line radioimmunotherapy candidate for the treatment of prostate cancer. Key differences between 177Lu-rosopatamab and 177Lu-vipivotide are highlighted in the following table:
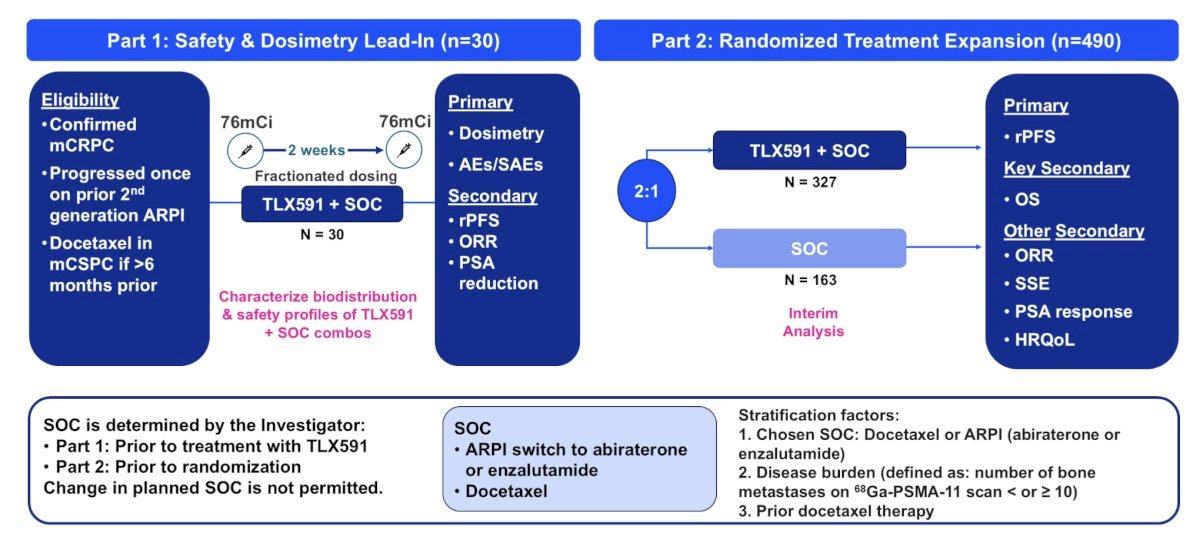
This multinational, multicenter, prospective, randomized, open label phase 3 study will have 2 parts: a dosimetry and safety lead-in (n = 30) and a randomized treatment expansion (n = 490). In Part 1, patients will be divided into 3 groups (n = 10 each) to receive two single IV injections of 76 millicuries (mCi) each, 14 days apart, of 177Lu-rosopatamab with best standard of care combinations with abiraterone, enzalutamide, or docetaxel to fully characterize biodistribution and safety profiles of 177Lu-DOTA-rosopatamab + standard of care combinations. Standard of care received will be determined prior to treatment with 177Lu-rosopatamab.
In Part 2, patients will be enrolled in a 2:1 ratio to receive either the best standard of care or two single IV injections of 76 mCi each (equivalent to a 45 mCi/m2 dose in a standard 1.7m2 individual) of 177Lu-rosopatamab, given 14 days apart, plus best standard of care. Standard of care will be determined prior to randomization, and a change in planned standard of care will not be permitted:
Eligible patients must have PSMA-expressing mCRPC that has progressed despite prior therapy with either enzalutamide or abiraterone plus prednisone, and one line of prior taxane therapy or have refused or are ineligible for taxanes. Patients must have adequate organ function, including at least 150 x 109/L platelets, hemoglobin 10 g/dL, and have PSMA-positive disease on 68Ga-PSMA-11 PET/CT imaging as confirmed by a central reader.
Key exclusion criteria include: (i) small cell histology, (ii) increased risk of hemorrhage or bleeding, (iii) known brain or hepatic metastases, (iv) history of stroke, (v) seizure, or (vi) treatment with radioisotopes within 6 months prior to randomization.
The primary endpoint is radiographic progression-free survival, and a key secondary endpoint is overall survival. Additional secondary endpoints include 5-year overall survival, tumor objective response rate, time to symptomatic skeletal event, and health-related quality of life. This study is currently enrolling.
Presented by: Denise Guibault, Medical Science Liaison, Telix Pharmaceuticals
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.