(UroToday.com) The 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix between December 2 and December 5, 2025, was host to the Poster Session. Dr. Alan Bryce presented poster #176: Efficacy of rucaparib vs physician’s choice in patients with BRCA-mutated metastatic castration-resistant prostate cancer by age: results from the TRITON3 study.
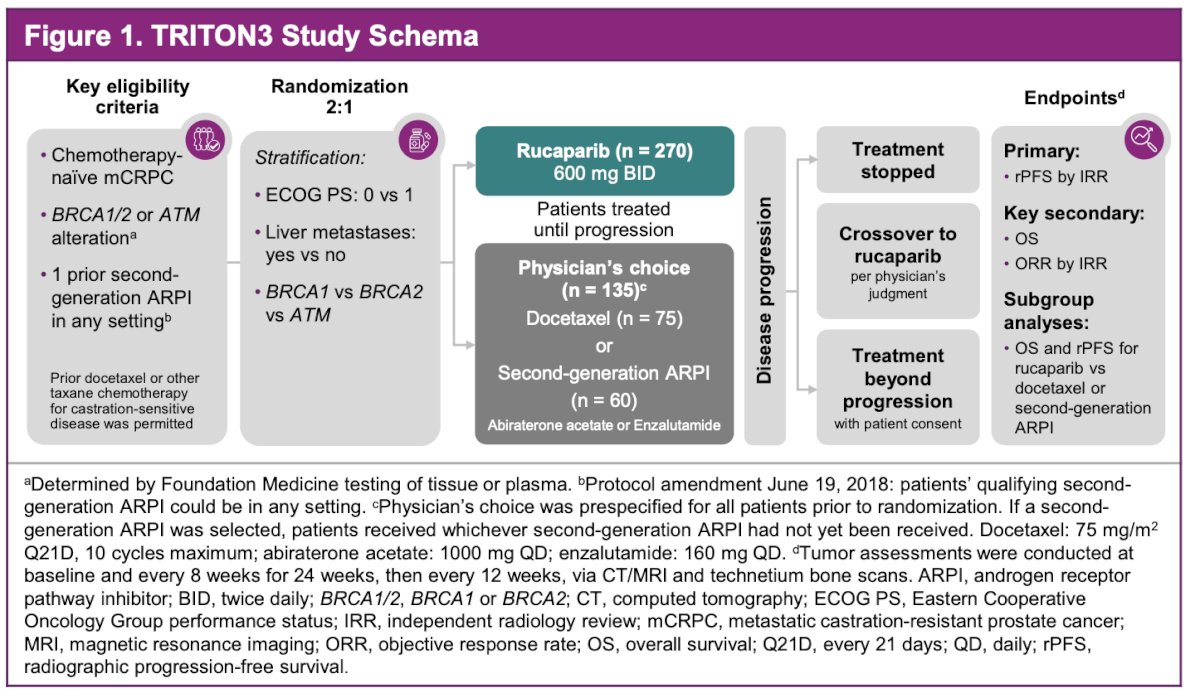
Dr. Bryce reviewed TRITON3, an open-label, randomized phase 3 trial evaluating rucaparib versus physician’s choice of therapy in men with mCRPC harboring BRCA1, BRCA2 or ATM alterations who had progressed on prior ARPI therapy.1 He noted, the control arm allowed either docetaxel or a second-generation ARPI. Notably, primary TRITON3 results showed a statistically significant rPFS improvement with the PARP inhibitor rucaparib in BRCA-mutated mCRPC. Given reports that poly(ADP-ribose) polymerase activity increases with age in men, particularly in those with prostate cancer, the investigators conducted an analysis to examine whether age influenced the clinical benefit observed with rucaparib.
For this exploratory work, men aged 18 or older with histologically or cytologically confirmed, chemotherapy-naïve mCRPC and a BRCA1, BRCA2 or ATM alteration were eligible, provided they had progressed after one prior second-generation ARPI. Patients were randomized 2:1 to rucaparib 600 mg twice daily or physician’s choice of therapy. The analysis focused on the BRCA1/2 cohort, stratified into three age groups younger than 65, 65 to 74, and 75 or older. The primary endpoint was rPFS, with an efficacy cut-off of August 25, 2022 and a safety cut-off of March 1, 2024. Treatment-emergent adverse events were reported across all age subgroups. The study schema is illustrated below.
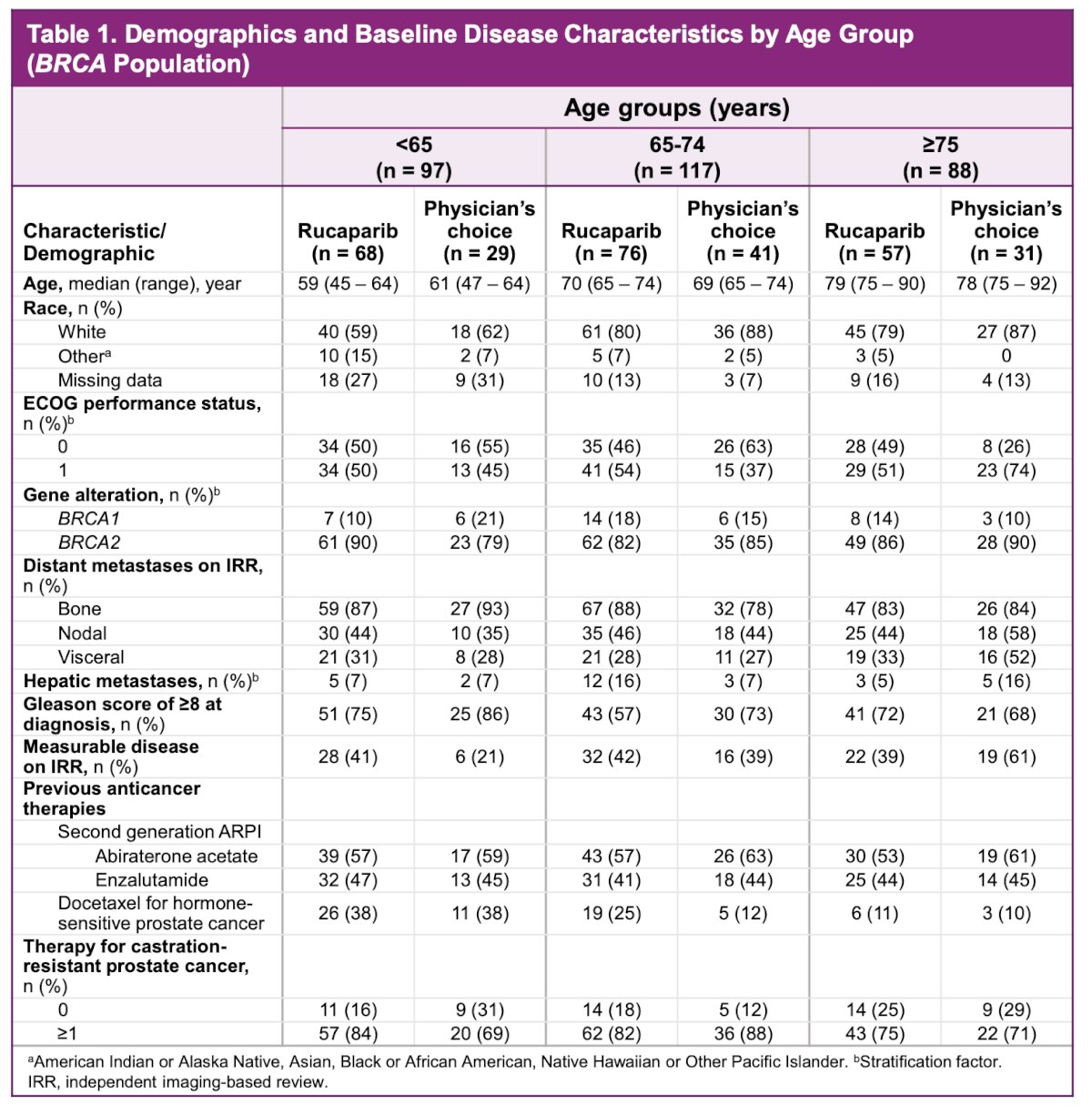
A total of 201 patients in the rucaparib arm and 101 in the physician’s choice arm with BRCA-mutated mCRPC were included in this age-based analysis. Baseline characteristics were generally balanced across the three age subgroups. Median age increased as expected across cohorts, and most patients had an ECOG performance status of 0 or 1. BRCA2 alterations predominated in all groups. Patterns of metastatic disease were similar, with bone involvement being most common and visceral metastases less frequent. Prior ARPI exposure reflected typical practice, with use of either abiraterone or enzalutamide, and a minority had received prior docetaxel for hormone-sensitive disease. Gleason score distributions and rates of measurable disease were consistent across age categories, supporting comparability of the populations included in this analysis.
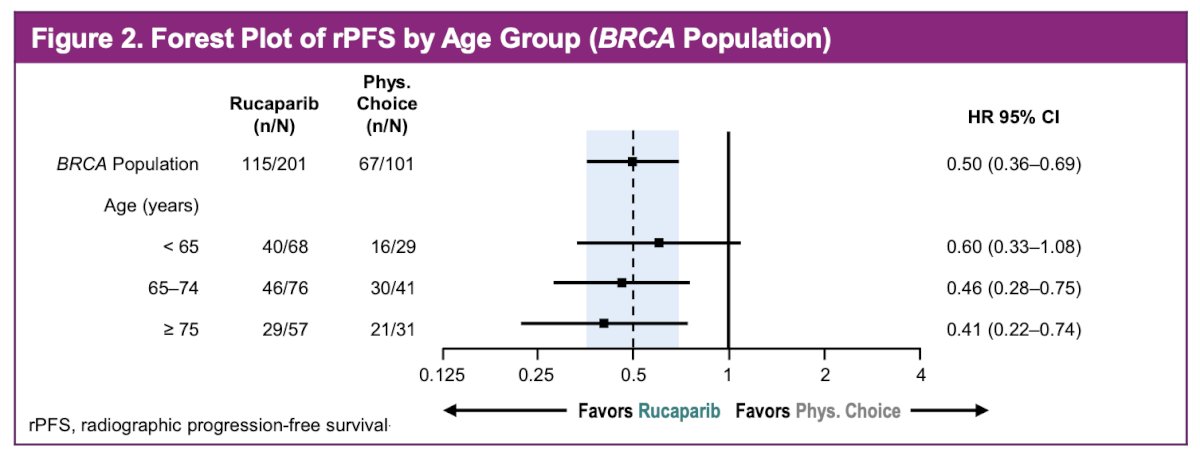
In the overall BRCA-mutated population, rucaparib continued to demonstrate a meaningful rPFS advantage, with a median rPFS of 11.2 months versus 6.4 months with physician’s choice of therapy, corresponding to an HR of 0.50 (95 percent CI, 0.36 to 0.69). The forest plot showed consistent benefit across all age groups. Patients younger than 65 derived benefit, although with a wider confidence interval, while those aged 65 to 74 and those 75 or older experienced more pronounced and statistically robust improvements. The treatment effect consistently favored rucaparib across each predefined age category.
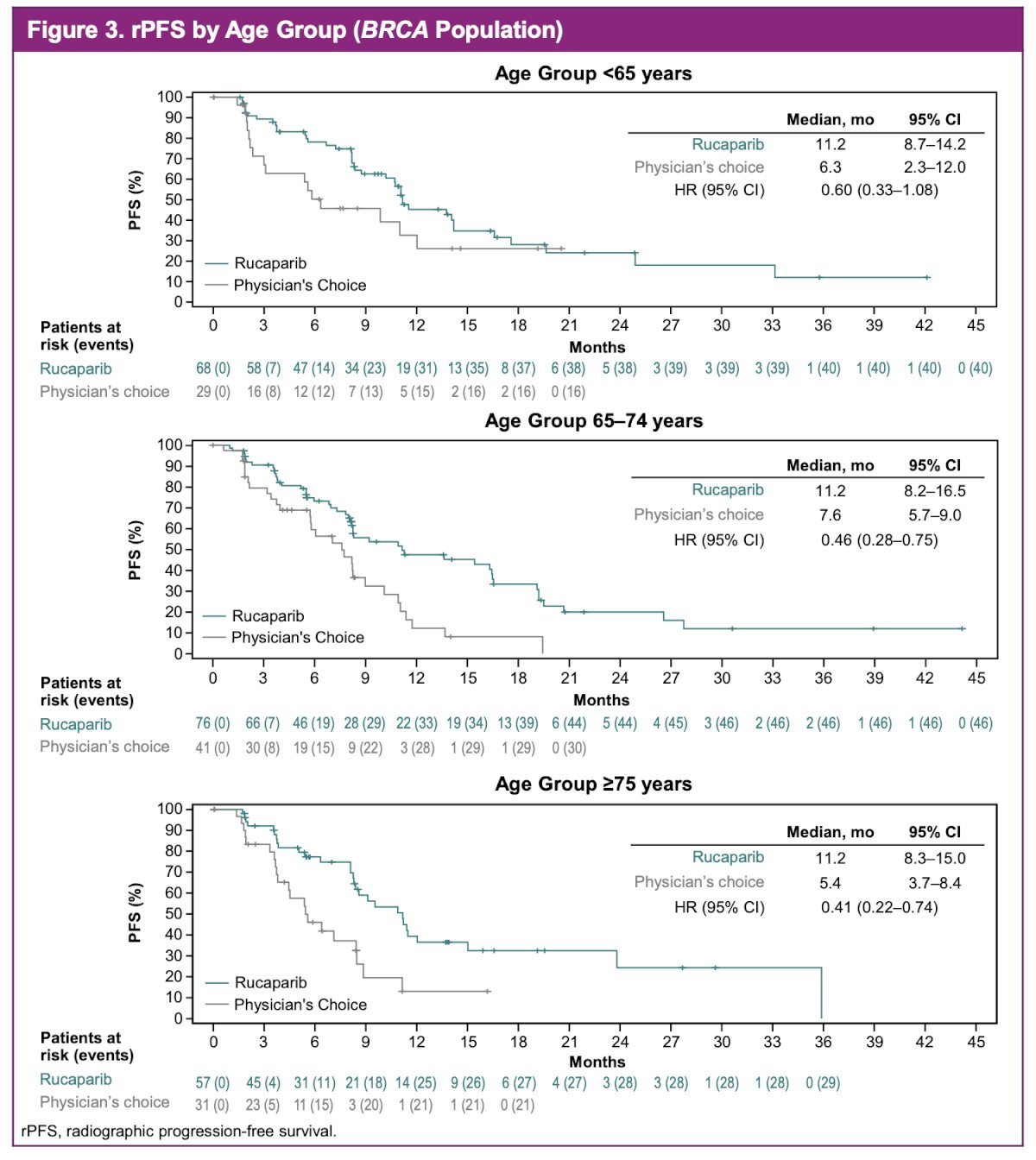
Across all three age cohorts, rucaparib consistently separated from physician’s choice early and maintained that separation over time. In patients younger than 65, median rPFS was 11.2 months with rucaparib versus 6.3 months with physician’s choice. A similar pattern was seen in those aged 65 to 74, with median rPFS of 11.2 versus 7.6 months, and in patients 75 or older, where rucaparib achieved a median rPFS of 11.2 months compared with 5.4 months. The curves showed durable benefit in each subgroup, including the oldest patients, with hazard ratios numerically improving with advancing age. Notably, for patients ≥75 years, rucaparib reduced the risk of progression by 59%.
In an additional exploratory look at the oldest patients, those aged 81 years or older, rucaparib continued to show meaningful activity. In this small subgroup, rucaparib reduced the risk of progression by 64 percent compared with physician’s choice of therapy, with a HR of 0.36 (95 percent CI, 0.13 to 0.97). Although numbers were limited, with 20 patients in the rucaparib arm and 10 in the physician’s choice arm, the treatment effect remained directionally consistent with the broader BRCA-mutated population.
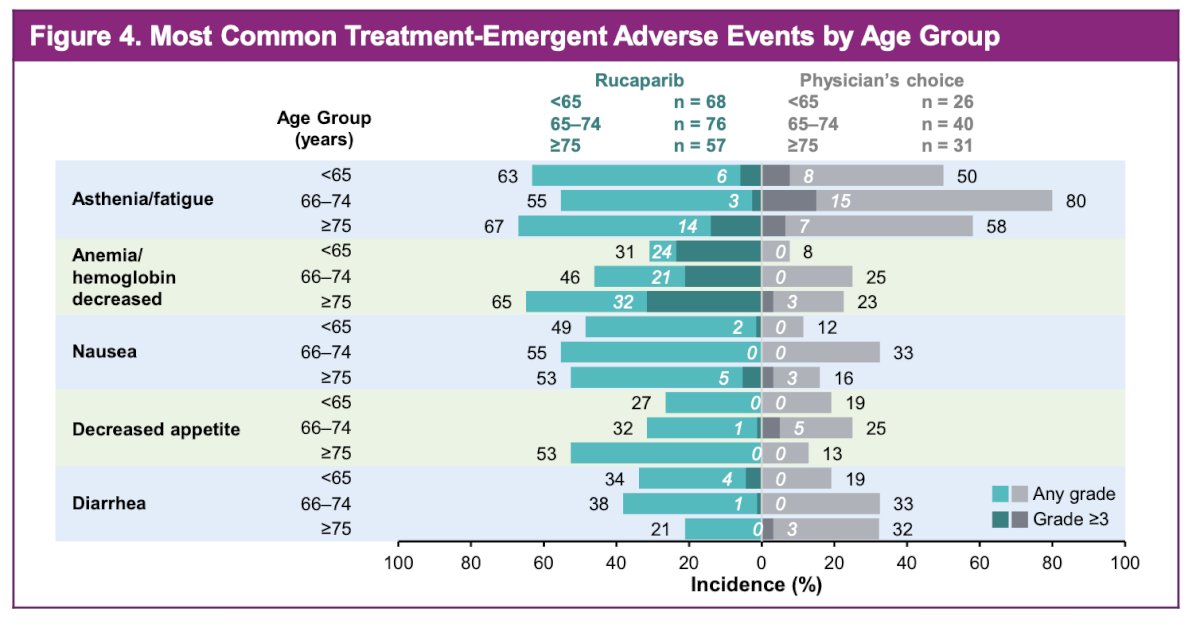
The most common TEAEs with rucaparib were asthenia or fatigue, anemia, and nausea, with similar event profiles across age groups. Anemia increased in frequency with advancing age in both treatment arms, and decreased appetite was more common among older patients receiving rucaparib. Other adverse events did not show clear age-related trends. Grade 3 or higher asthenia or fatigue and anemia were most frequent in the oldest rucaparib subgroup, although the overall safety profile remained consistent with prior reports.
Dr Bryce concluded that rucaparib provided a consistent rPFS benefit across all age groups, including in the oldest patients evaluated. The safety profile remained generally similar regardless of age, with no unexpected signals. Taken together, these findings support the use of rucaparib for patients with BRCA-mutated mCRPC independent of age.
Presented by: Alan H. Bryce, MD, Medical Director of the Genomic Oncology Clinic at Mayo Clinic, Arizona, United States of America.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Penn State Health, @chavarriagaj on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References: