(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a prostate cancer poster session. Dr. Benjamin Lowentritt presented the results of a real-world study comparing PSA responses among patients with metastatic castration-sensitive prostate cancer (mCSPC) treated with apalutamide versus abiraterone acetate.
Next generation androgen receptor pathway inhibitors (ARPIs), apalutamide and abiraterone acetate, are approved for use in combination with androgen deprivation therapy (ADT) for the treatment of mCSPC.1,2 In phase III trials, early and sustained PSA reduction of ≥90% (PSA90) following treatment initiation has been linked to improved prognosis among patients with mCSPC who initiated treatment with apalutamide (TITAN)3 and abiraterone acetate (LATITUDE).4
In a retrospective study using United States (US) community-based urology electronic medical record (EMR) data, apalutamide was associated with a significantly higher proportion of patients achieving PSA90 response compared to abiraterone acetate in patients with mCSPC with confirmed in-office medication dispensing.5 To build upon prior real-world evidence,6 this study evaluated PSA90 response among mCSPC patients initiated on apalutamide or abiraterone acetate at 6 months using EMR supplemented with insurance claims data.
This retrospective study used de-identified clinical data from the Precision Point Specialty (PPS) Analytics database, representing >90 U.S. community urology practices, linked with administrative claims from the Komodo Research Database (KRD+). The study period spanned September 17, 2018, to December 31, 2023. Patients were ARPI-naïve at baseline.
Patients were assigned to mutually exclusive treatment cohorts based on their first dispensation or paid pharmacy claim for apalutamide or abiraterone acetate. The index date was the first such claim occurring on or after September 17, 2019 (the FDA approval date for apalutamide).1 Baseline characteristics were assessed in the 12 months prior to index. Follow-up continued until treatment discontinuation (defined by a ≥90-day gap), non-index ARPI initiation, radiopharmaceutical therapy, loss of clinical activity, or end of data availability.
mCSPC status was determined using diagnosis codes or EMR-abstracted indicators of bone, nodal, or visceral metastases without prior castration resistance. Castration resistance was defined using a previously validated algorithm incorporating ADT records and PSA trajectory.⁷ Patients in the abiraterone acetate cohort were not required to have concurrent prednisone.
The primary outcome was PSA90 (≥90% PSA decline from baseline) within 6 months. To control for baseline differences, inverse probability of treatment weighting (IPTW) using propensity scores was performed following established methodological standards.⁸⁻⁹ Weighted Kaplan-Meier and Cox proportional hazards models estimated PSA90 rates and hazard ratios (HRs).
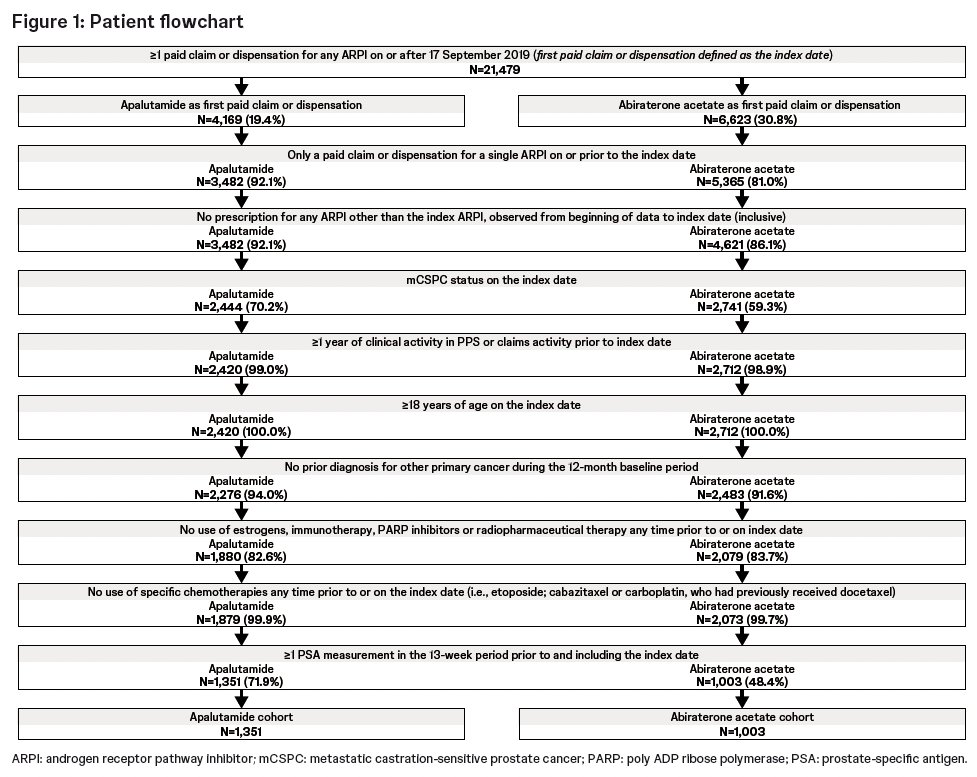
After applying all inclusion and exclusion criteria, 1,351 apalutamide-treated and 1,003 abiraterone acetate-treated mCSPC patients were included. The study flow chart is illustrated below:
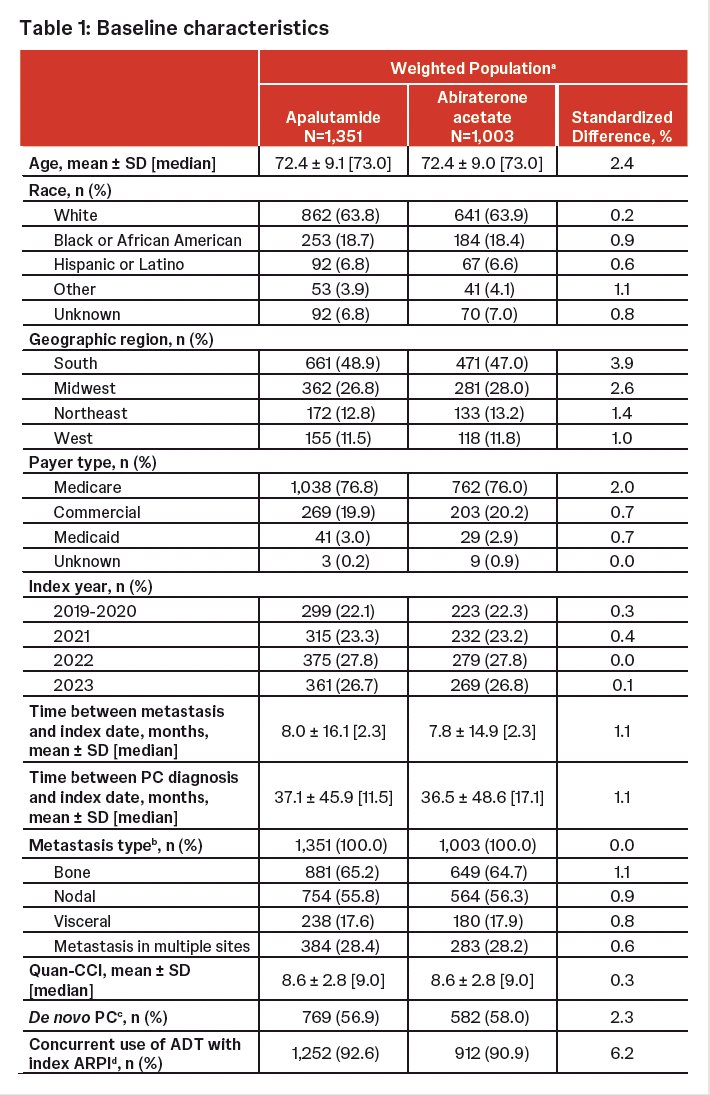
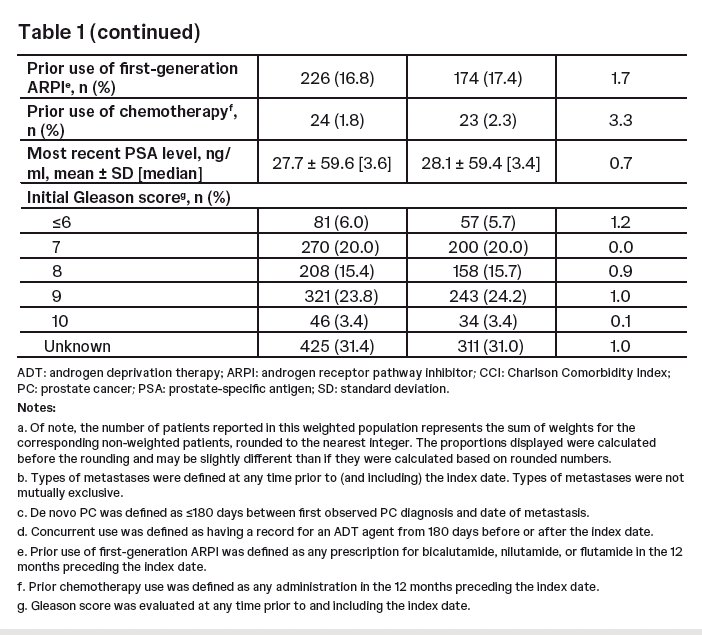
The key baseline cohort characteristics were as follows:
- Mean age: 72.4 years in both cohorts
- Race: ~64% White, ~19% Black, ~7% Hispanic
- Geographic distribution: ~49% South, ~27% Midwest, remainder Northeast/West
- ADT overlap with index: 92.6% for apalutamide, 90.9% for abiraterone acetate
- Metastatic patterns: bone (65%), nodal (56%), visceral (18%), multiple sites (~28%)
- Baseline PSA: median 3.6 ng/mL (apalutamide) and 3.4 ng/mL (abiraterone acetate)
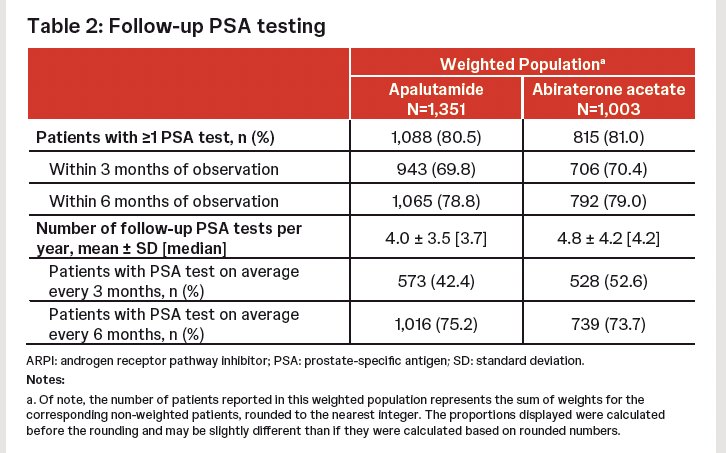
PSA monitoring during follow-up was similar, with ~80% of patients in each cohort having ≥1 follow-up PSA test and mean frequency of 4–4.8 PSA tests per year.
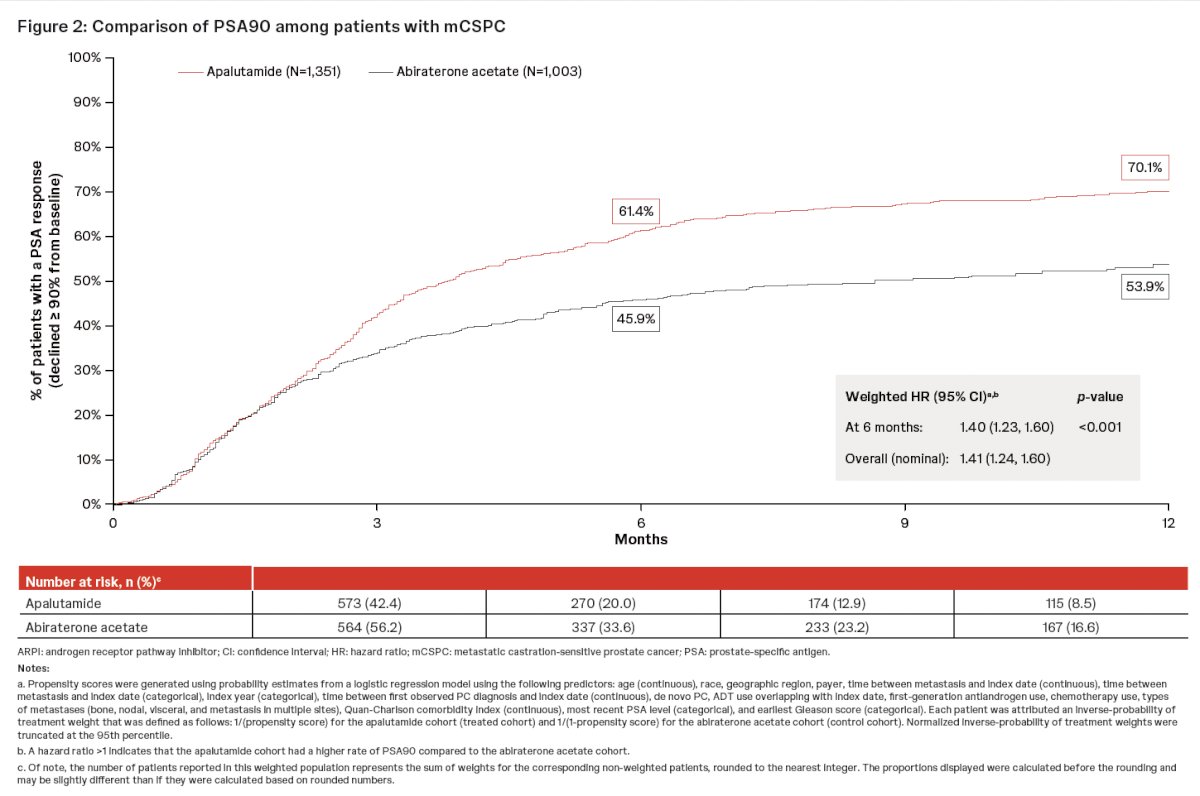
Apalutamide was associated with significantly higher and earlier PSA90 responses, compared to abiraterone acetate:
- At 6 months:
- PSA90: 61.4% (apalutamide) vs 45.9% (abiraterone acetate)
- Weighted HR: 1.40 (95% CI: 1.23–1.60; p<0.001)
- Median time to PSA90:
- 3.8 months with apalutamide
- 8.7 months with abiraterone acetate
These findings were consistent in the nominal (non-IPTW) analysis as well (HR 1.41).
The PSA surveillance practices appeared clinically consistent between groups:
- Testing within 3 months: 69.8% (apalutamide) vs 70.4% (abiraterone acetate)
- Testing within 6 months: 78.8% vs 79%
- Average PSA testing every 3 months: 42.4% vs 52.6%
Key limitations include the following:
- Potential misclassification due to reliance on EMR and administrative claims
- Abiraterone acetate’s indication for high-risk mCSPC may lead to residual differences even after IPTW
- Residual confounding remains possible because regression methods can only adjust for measured covariates
- PSA testing frequency was not mandated, introducing variability in assessment timing
Dr. Lowentritt concluded as follows:
- A significantly higher proportion of ARPI-naïve mCSPC patients achieved PSA90 by 6 months with apalutamide versus abiraterone acetate.
- Earlier deep PSA responses were observed with apalutamide, with a median time-to-PSA90 nearly five months shorter than with abiraterone acetate.
- These findings may hold important long-term clinical significance, given the established association between early PSA kinetics and survival outcomes in mCSPC.
- Real-world evidence from this large, linked EMR–claims dataset supports potential therapeutic advantages of apalutamide in routine U.S. practice.
Presented by: Benjamin H. Lowentritt, MD, FACS, Urologist, Chesapeake Urology Associates PA, Baltimore, MD
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References:
- U.S. Food and Drug Administration. FDA approves apalutamide for metastatic castration-sensitive prostate cancer. 2022.
- U.S. Food and Drug Administration. FDA approves abiraterone acetate in combination with prednisone for high-risk metastatic castration-sensitive prostate cancer. 2022.
- Chowdhury S, Davis ID, Jones RJ, et al. Apalutamide in metastatic castration-sensitive prostate cancer: PSA response and outcomes from TITAN. Ann Oncol. 2023; 34(5):477–485.
- Matsubara N, Kakehi Y, Akaza H, et al. Early PSA response and prognosis in abiraterone-treated mCSPC (LATITUDE). Clin Trial. 2020; 77(4):494–500.
- Lowentritt B, Bilen MA, Pilon D, et al. Real-world PSA90 response: Apalutamide vs abiraterone acetate in mCSPC. Urol Oncol. 2023; 41(5):252.e19–252.e27.
- U.S. Food and Drug Administration. Considerations for the Use of Real-World Data and Evidence in Drug Regulatory Decision-Making. 2021.
- Freedland SJ, Tutrone R, De Hoedt A, et al. Identifying castration resistance in clinical practice: EMR-based algorithm. Curr Med Res Opin. 2021; 37(4):609–622.
- Austin PC. An introduction to propensity score methods for reducing confounding in observational studies. Multivariate Behav Res. 2011; 46(3):399–424.
- Austin PC. Balance diagnostics for comparing weighted cohorts. Stat Med. 2009; 28(25):3083–3107.