(UroToday.com) The 2025 Society of Urologic Oncology (SUO) annual meeting, held in Phoenix between December 2 and December 5, 2025, was host to the Poster Session. Dr. Sabree Burbage presented poster #114: Healthcare resource utilization and medical costs in patients with metastatic castration sensitive prostate cancer initiating apalutamide or darolutamide in the United States.
Dr Burbage noted that real-world studies have demonstrated improved clinical outcomes and lower medical costs for patients with metastatic castration-sensitive prostate cancer treated with apalutamide compared with enzalutamide or abiraterone acetate. Despite its growing use, data characterizing healthcare resource utilization and associated costs for darolutamide in routine practice remain limited. This study aimed to address that gap by evaluating real-world HRU and costs among patients with mCSPC treated with either apalutamide or darolutamide.
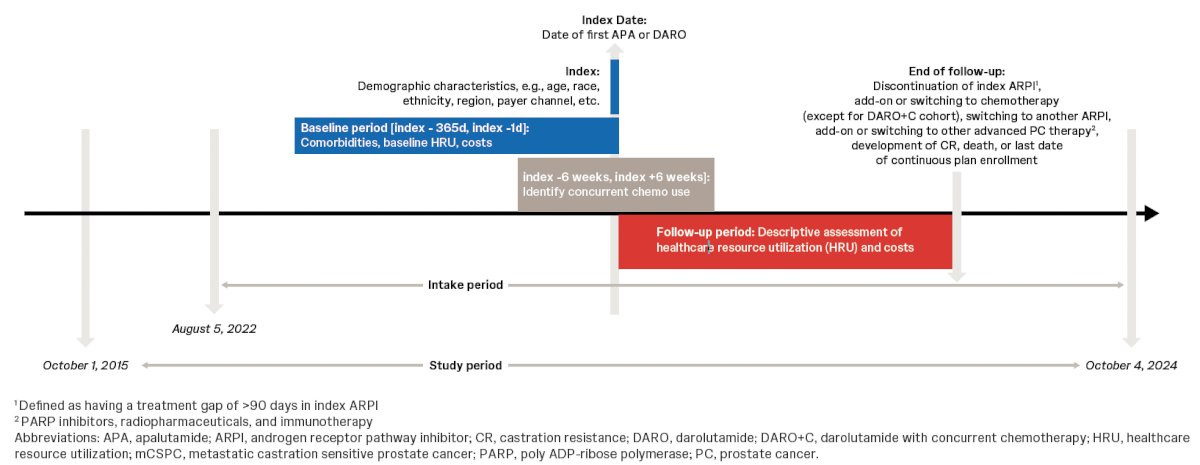
The investigators performed a retrospective descriptive analysis using healthcare claims from the Komodo Research Dataset. Eligible patients had mCSPC and initiated apalutamide or darolutamide on or after August 5, 2022, with at least 12 months of continuous insurance enrollment before treatment. For those starting darolutamide, cohorts were further stratified based on receipt of concurrent chemotherapy. Patients were followed from the index date until the earliest of ARPI discontinuation, addition or switch to chemotherapy, transition to another ARPI or other advanced prostate cancer therapy, progression to castration resistance, death, loss of continuous enrollment, or the end of data availability on October 4, 2024. Notably, all-cause and prostate cancer–related healthcare utilization and per-patient-per-year medical costs were assessed by the investigators during both baseline and follow-up. The study design is shown below.
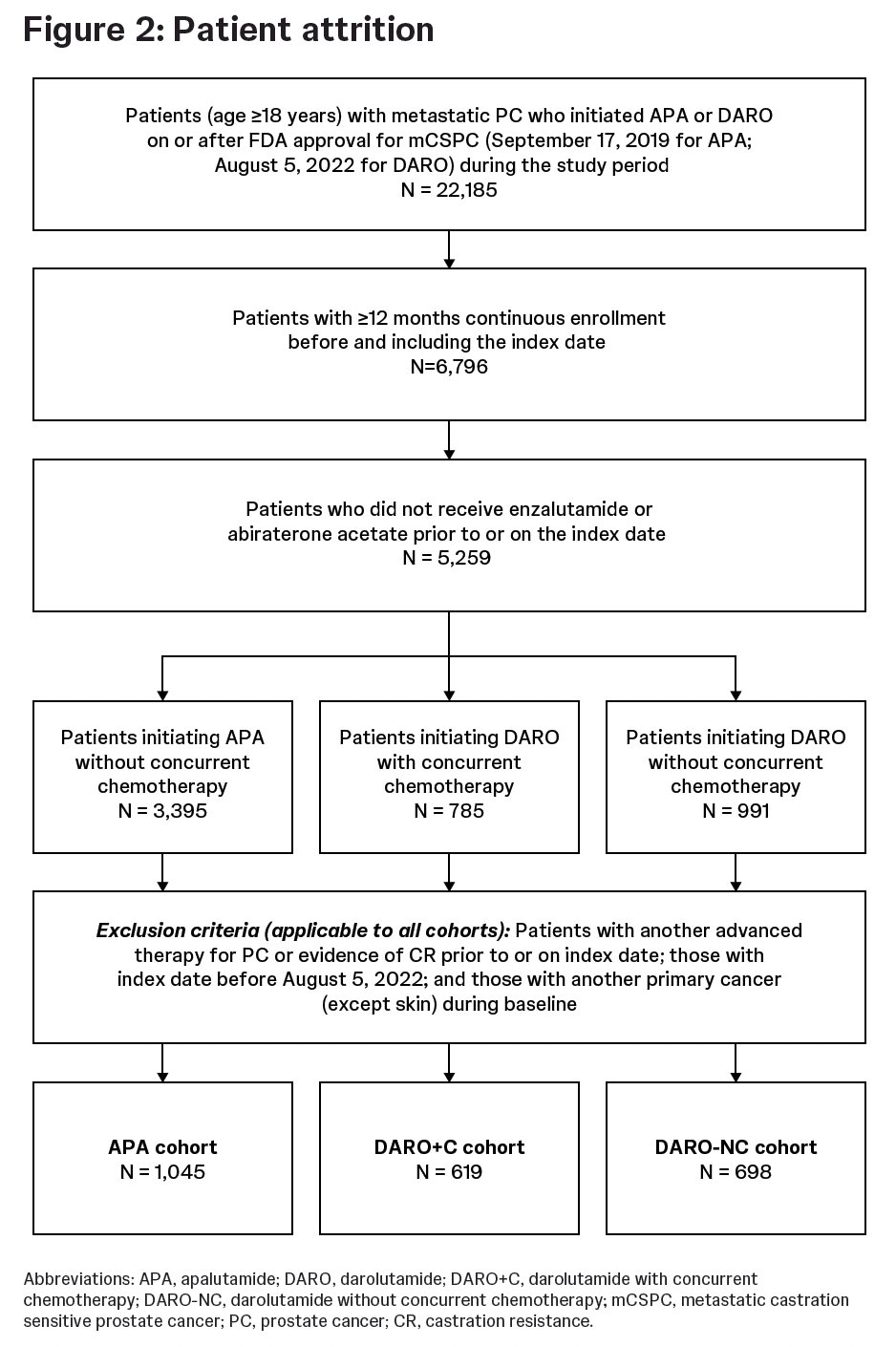
Among patients with mCSPC, 1045 initiated apalutamide and 1317 initiated darolutamide, with nearly half (47%) of the darolutamide cohort receiving concurrent chemotherapy as illustrated in the graphic below.
Patient demographics and clinical characteristics are summarized in the table below. The mean age at diagnosis varied across cohorts 71.9 years in the APA cohort, 63.8 years in the DARO+C cohort, and 68.5 years in the DARO-NC cohort. Insurance profiles also differed: most APA patients had Medicare (61.6%), while the majority of DARO+C patients were commercially insured (59.9%); the DARO-NC cohort was more evenly split between Medicare (48.6%) and commercial insurance (42.3%). De novo mCSPC was common across groups, highest in the DARO+C cohort (90.0%), followed by DARO-NC (75.1%) and APA (66.4%), with most patients receiving concurrent ADT (87.7%, 96.9%, and 84.7%, respectively). Bone metastases were the predominant metastatic site in all cohorts, and visceral involvement was observed in 9.4% of APA, 16.5% of DARO+C, and 13.5% of DARO-NC patients.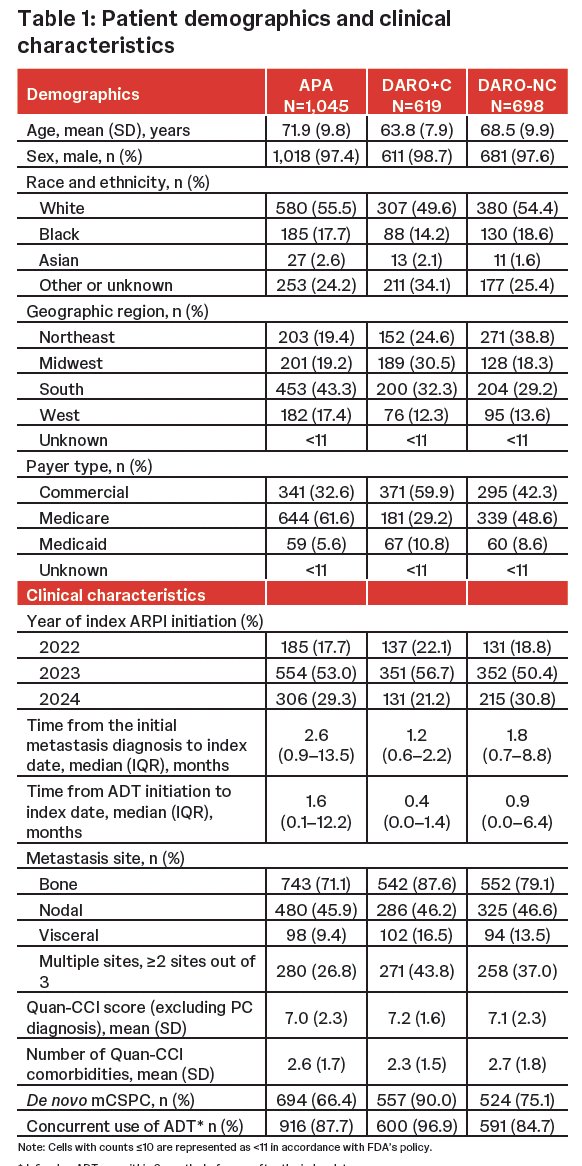
The mean follow-up was 5.4 months for the APA cohort, 6.7 months for the DARO+C cohort, and 5 months for the DARO-NC cohort. The table below summarizes all-cause and prostate cancer-related healthcare resource utilization across subgroups.
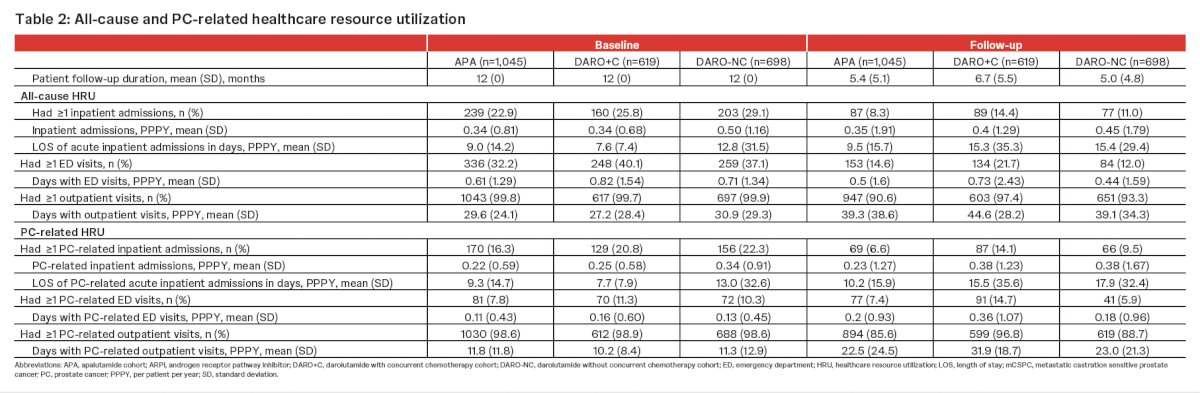
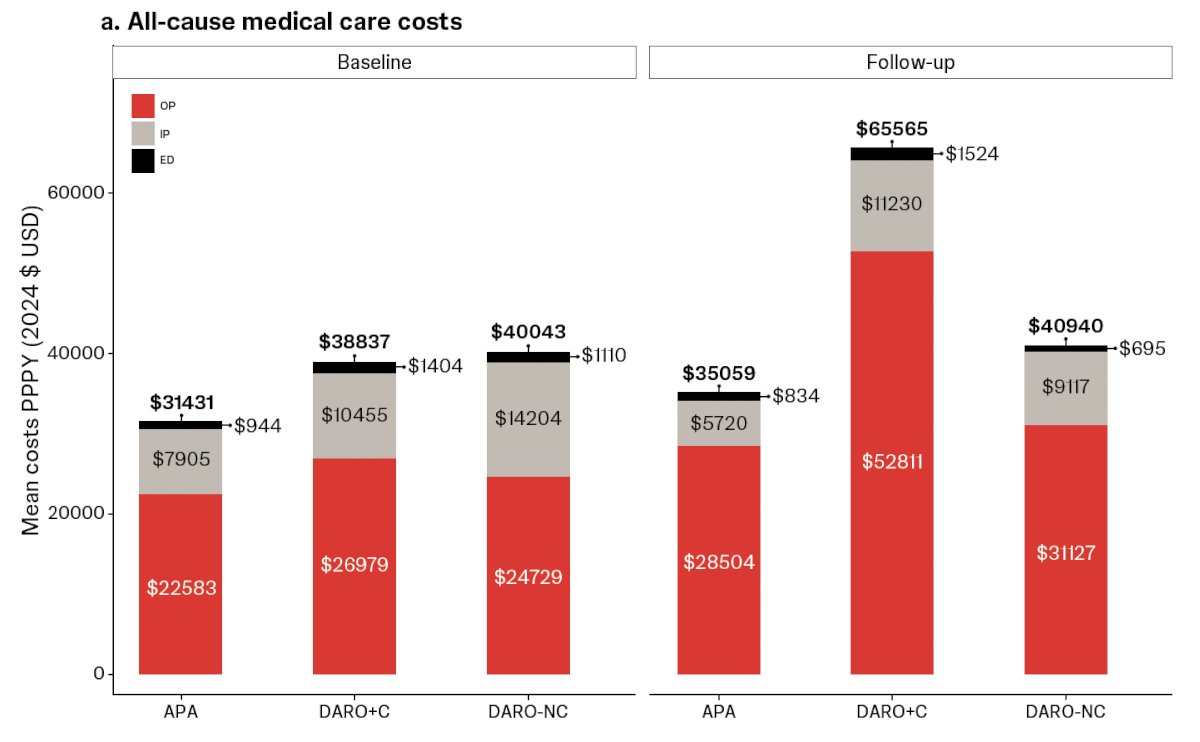
During follow-up, prostate cancer–related inpatient admissions were more frequent among patients treated with darolutamide, particularly those receiving concurrent chemotherapy, occurring in 14.1% of the DARO+C cohort compared with 9.5% of DARO-NC (Darolutamide no-chemotherapy) and 6.6% of the apalutamide group. Among those hospitalized, the mean length of stay for PC-related acute admissions was longest in the DARO-NC cohort at 17.9 days per patient-year, followed by 15.5 days in DARO+C and 10.2 days in the apalutamide cohort. These differences in hospitalization rates and duration contributed to higher overall all-cause medical care costs during follow-up, with the DARO+C group demonstrating the highest per-patient-per-year expenditure as shown in the figure below.
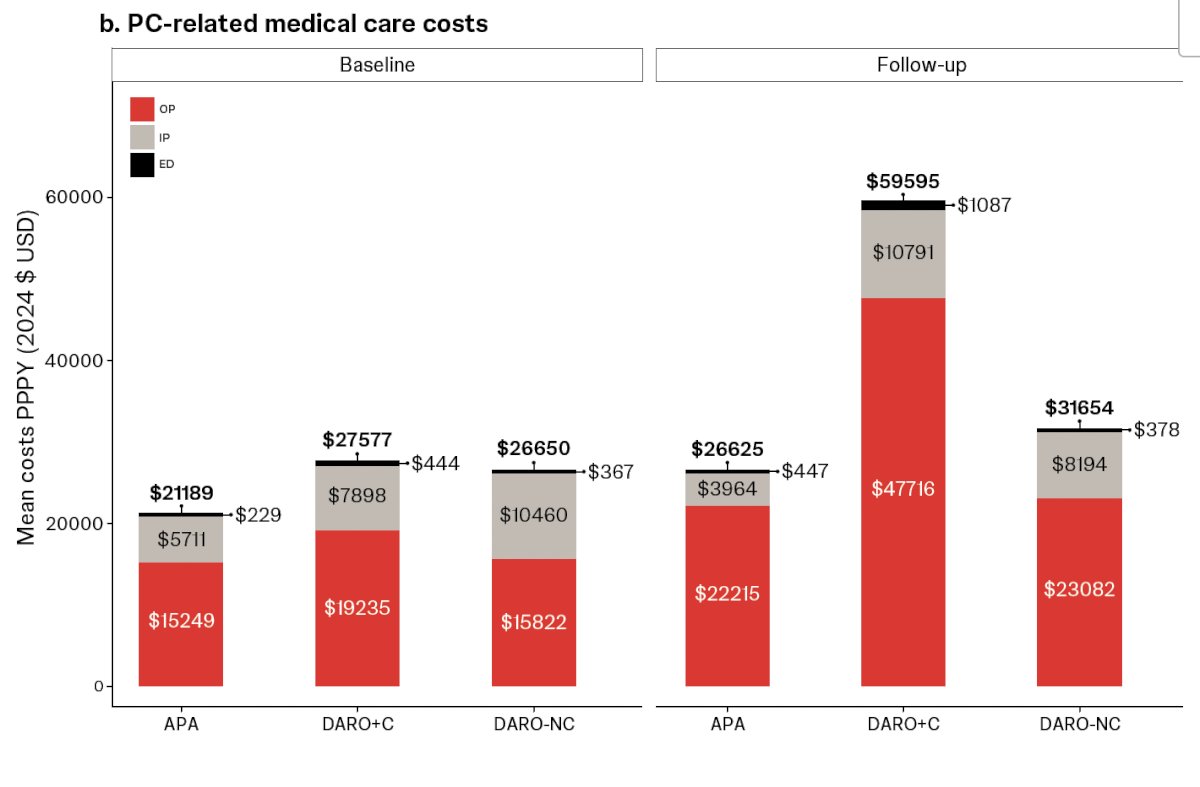
Moreover, PC-related medical costs per patient per year were lowest for apalutamide at $26,625, higher for darolutamide without chemotherapy at $31,654, and highest for patients receiving darolutamide with concurrent chemotherapy at $59,595.
Lastly, the study has several limitations. As a claims-based analysis, the database may contain inaccuracies, and patient histories may be incomplete. Cost estimates were generated using Komodo’s proprietary algorithms, which may not fully reflect the actual costs incurred in clinical practice. In addition, defining treatment cohorts using a 6-week post-index window may introduce immortal-time bias, particularly in the ARPI plus chemotherapy subgroup.
Dr. Burbage concluded the presentation with the following key takeaways:
- Post-index annual healthcare utilization and medical costs varied meaningfully across treatment groups, with the highest levels seen in patients receiving darolutamide with concurrent chemotherapy, followed by darolutamide alone, then apalutamide.
- These cost differences may reflect underlying clinical differences between cohorts, including disease severity and treatment patterns.
- Further adjusted analyses in balanced patient groups are needed to more accurately characterize HRU and costs among patients with mCSPC initiating ARPIs.
Presented by: Sabree Burbage, PharmD, MPH, Population Health Research, Janssen Scientific Affairs, LLC, Horsham, PA, USA.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Penn State Health, @chavarriagaj on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.