The 2025 SUO annual meeting featured a late-breaking abstract session and a presentation by Dr. Lorraine Scanlon discussing a comparative cohort study assessing relief of venous congestion as a modifiable cause of renal dysfunction in renal cell carcinoma (RCC) with IVC tumor thrombus.
RCC with IVC tumor thrombus is often associated with poor eGFR at baseline, yet many patients recover renal function post-operatively. As such, this pattern does not fit with structural or irreversible chronic kidney disease. The traditional acute kidney injury framework is as follows:
- Pre-renal: decrease perfusion
- Intrinsic: nephron injury
- Post-renal: obstruction that leads to hydronephrosis
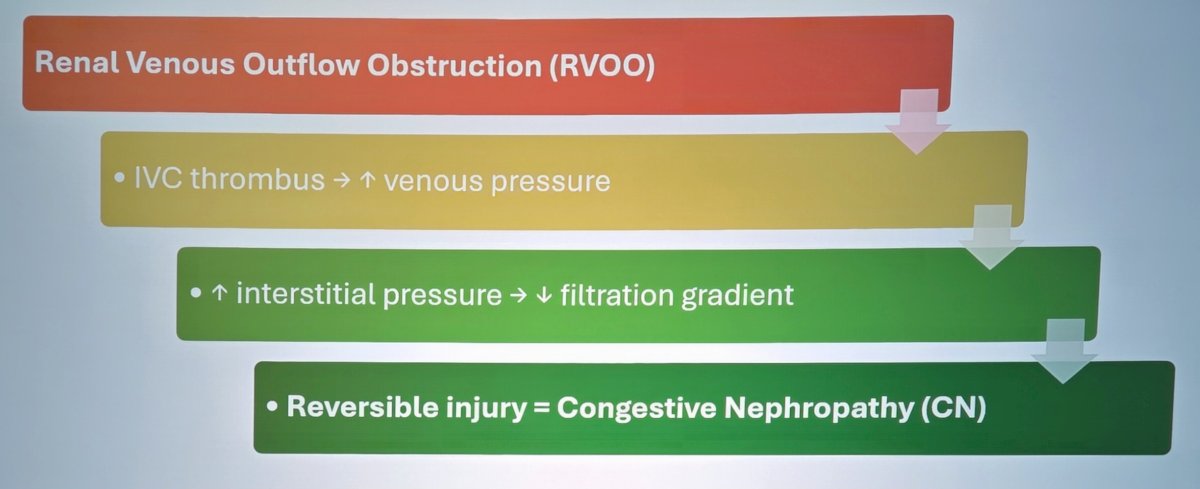
Dr. Scanlon emphasized that IVC tumor thrombus does not fit this framework, given that there is normal arterial flow, no parenchymal injury, and no ureteric obstruction; thus, there are no pre-renal, intrinsic, or post-renal injuries. A fourth mechanism present in IVC tumor thrombus patients may include renal venous outflow obstruction from the IVC tumor thrombus, which increases venous pressure, leading to increased interstitial pressure, leading to a decreased filtration gradient. This results in a reversible injury: congestive nephropathy
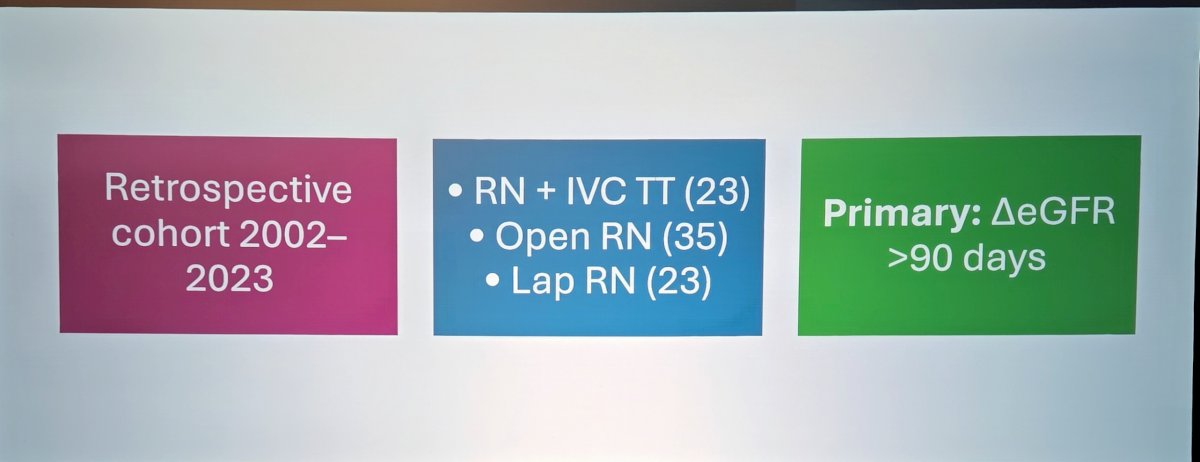
The hypothesis for this study is that relieving the venous congestion via a thrombectomy would lead to improved renal preservation despite worse baseline function. This was a retrospective cohort study from 2002 to 2023 for patients who underwent radical nephrectomy with IVC tumor thrombectomy (n = 23), open radical nephrectomy (n = 35), and laparoscopic radical nephrectomy (n = 23), with a primary outcome of change in eGFR after 90 days:
In terms of baseline differences between the patients, IVC tumor thrombus patients had larger tumors, higher ASA, and worse baseline eGFR. Post-operatively, all groups had a worsening in eGFR on post-operative days 1-2, but only the IVC tumor thrombus patients recovered eGFR after 90 days, suggesting reversible renal physiology. The absolute change in eGFR was:
- IVC tumor thrombus: -10
- Open radical nephrectomy: -25
- Laparoscopic radical nephrectomy -25
The percentage decline in eGFR was ~21% for IVC tumor thrombus patients and ~38% for those undergoing radical nephrectomy without IVC thrombectomy.
Dr. Scanlon concluded her presentation discussing a comparative cohort study assessing relief of venous congestion as a modifiable cause of renal dysfunction in RCC with IVC tumor thrombus, with the following take-home points:
- Renal injury in patients with IVC tumor thrombus is hemodynamic, not structural
- Congestive nephropathy reframes chronic kidney disease in the IVC thrombus setting
- This data supports timely IVC thrombectomy and introduces a fourth acute kidney injury mechanism
Presented by: Lorraine Scanlon, University of Western Ontario, London, Ontario, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.