(UroToday.com) The 2025 SUO annual meeting featured a late-breaking abstract session and a presentation by Dr. Lin Lin discussing a phase II trial of neoadjuvant stereotactic ablative radiotherapy for caval thrombus in newly diagnosed renal cell carcinoma (RCC). Notably, 4-10% of RCC patients develop IVC tumor thrombus, with the standard of care being radical nephrectomy with IVC thrombectomy +/- adjuvant therapy.
The perioperative mortality from this operation is up to 10.8% with 5-year cancer-specific survival rates of 25-53%. Stereotactic body radiotherapy offers the potential for a high dose of hypo-fractionated radiation, and a safety lead in trial of six patients receiving neoadjuvant stereotactic ablative body radiotherapy to the IVC tumor thrombus demonstrated safety and feasibility in the Neo-SAbR trial. The objective of this phase II trial was to assess the oncologic efficacy and long-term outcomes of neoadjuvant stereotactic ablative body radiotherapy for IVC tumor thrombus in patients with newly diagnosed RCC.
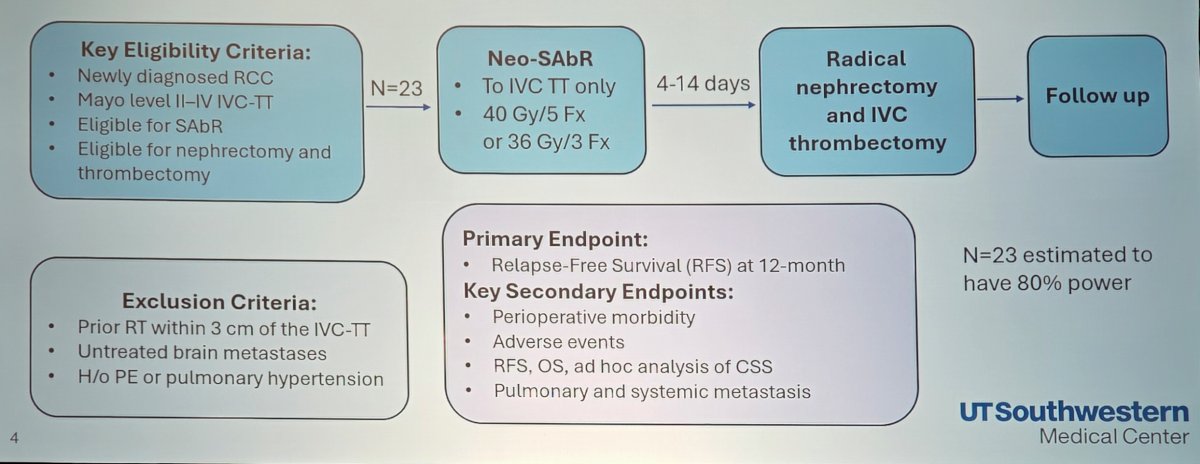
This was a prospective, single-center, safety-led, single-arm phase II trial, accruing newly diagnosed patients with RCC and Mayo level II-IV IVC tumor thrombus eligible for stereotactic ablative body radiotherapy, radical nephrectomy, and IVC thrombectomy. All patients received 40 Gy in 5 fractions or 36 Gy in 3 fractions of stereotactic ablative body radiotherapy, and 4-14 days later underwent radical nephrectomy and IVC thrombectomy. The primary endpoint was relapse-free survival at 12 months. The trial design is highlighted below:
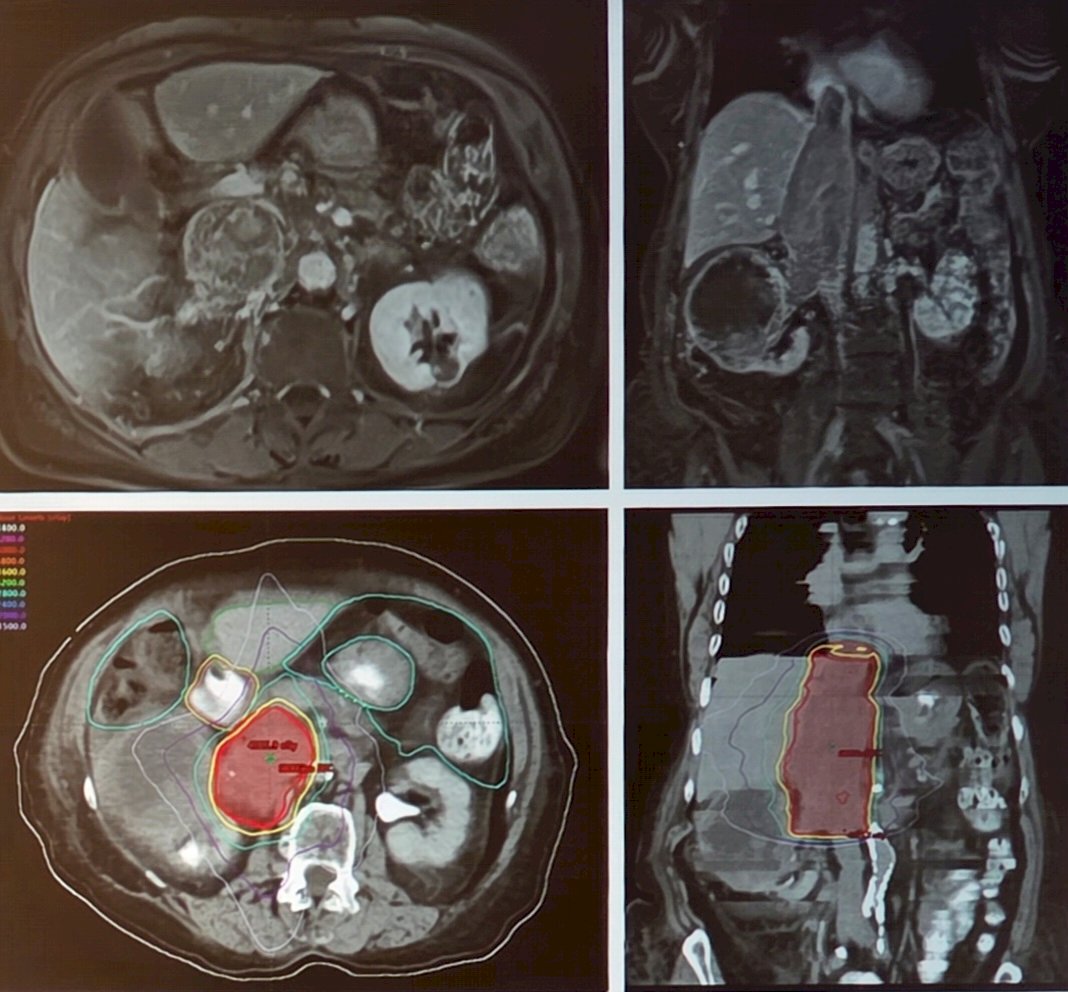
There were 23 patients enrolled between July 2015 and January 2024, with all patients receiving neoadjuvant stereotactic body radiotherapy to the IVC tumor thrombus. There were 22 patients that underwent surgery, with 1 patient being excluded secondary to widespread metastasis to the liver. Overall, 21 patients had follow-up, with 1 patient being excluded secondary to a perioperative death from COVID-19 pneumonia during the pandemic. The following figure highlights 36 Gy of radiotherapy in 3 fractions to the IVC tumor thrombus:
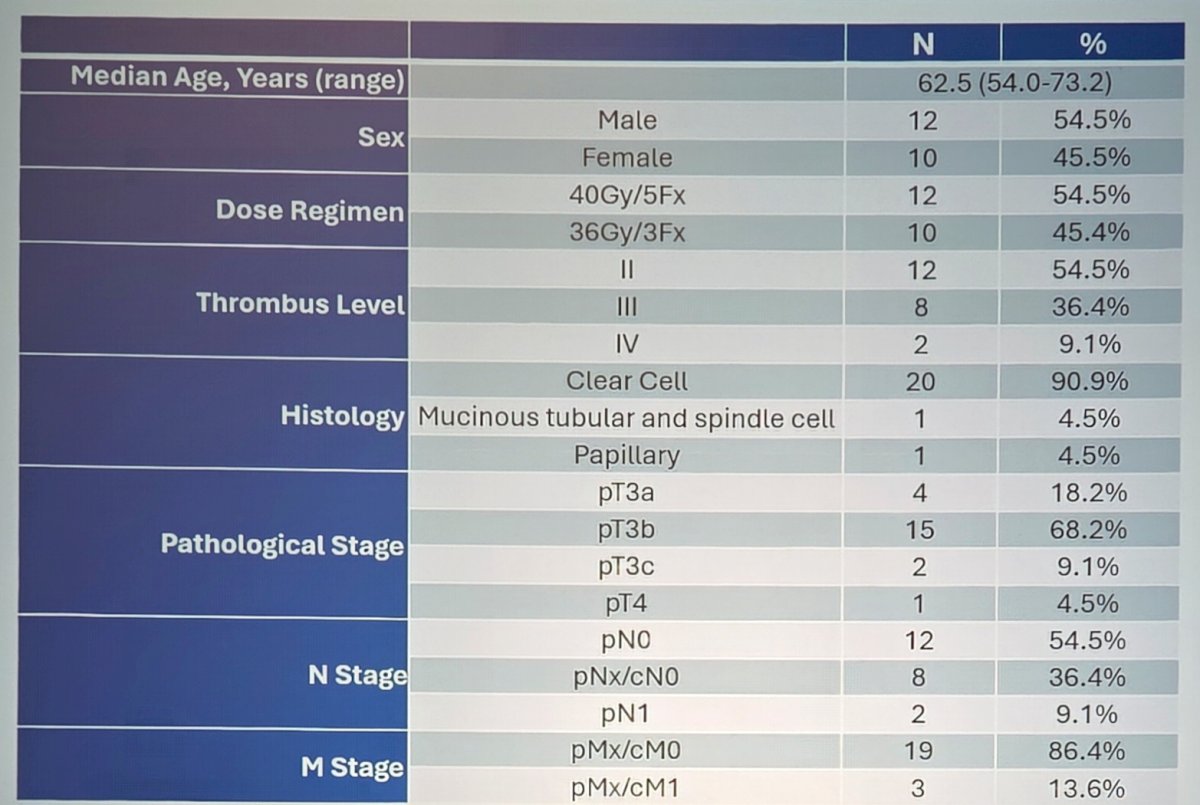
Among the 23 patients, the median age was 62.5 years (range: 54.0-73.2), 54.5% were male, 54.5% had level II IVC tumor thrombus, 90.9% had clear cell histology, 68.2% were pT3b, 9.1% had pN1, and 86.4% had pMx/cM0:
Surgical outcomes were as follows:
- Thrombi down-staging: n = 5 (22.7%)
- Cardiopulmonary bypass and thoracotomy: n = 3 (13.6%)
- Median case duration: 217.5 min (range: 115-478)
- Median estimated blood loss: 800 mL (range: 100-10,000)
- Intraoperative transfusion: n = 14 (63.6%)
- Perioperative mortality: n = 0
- Clavien-Dindo III-IV: n = 3 (13.6%)
- Median hospital length of stay: n = 4 days (range: 2-63)
Over a median follow-up of 35.2 months, the recurrence-free survival at 12 months was 71.4% (80% CI 56.6 – 82.0%; p = 0.087, alpha = 0.20):
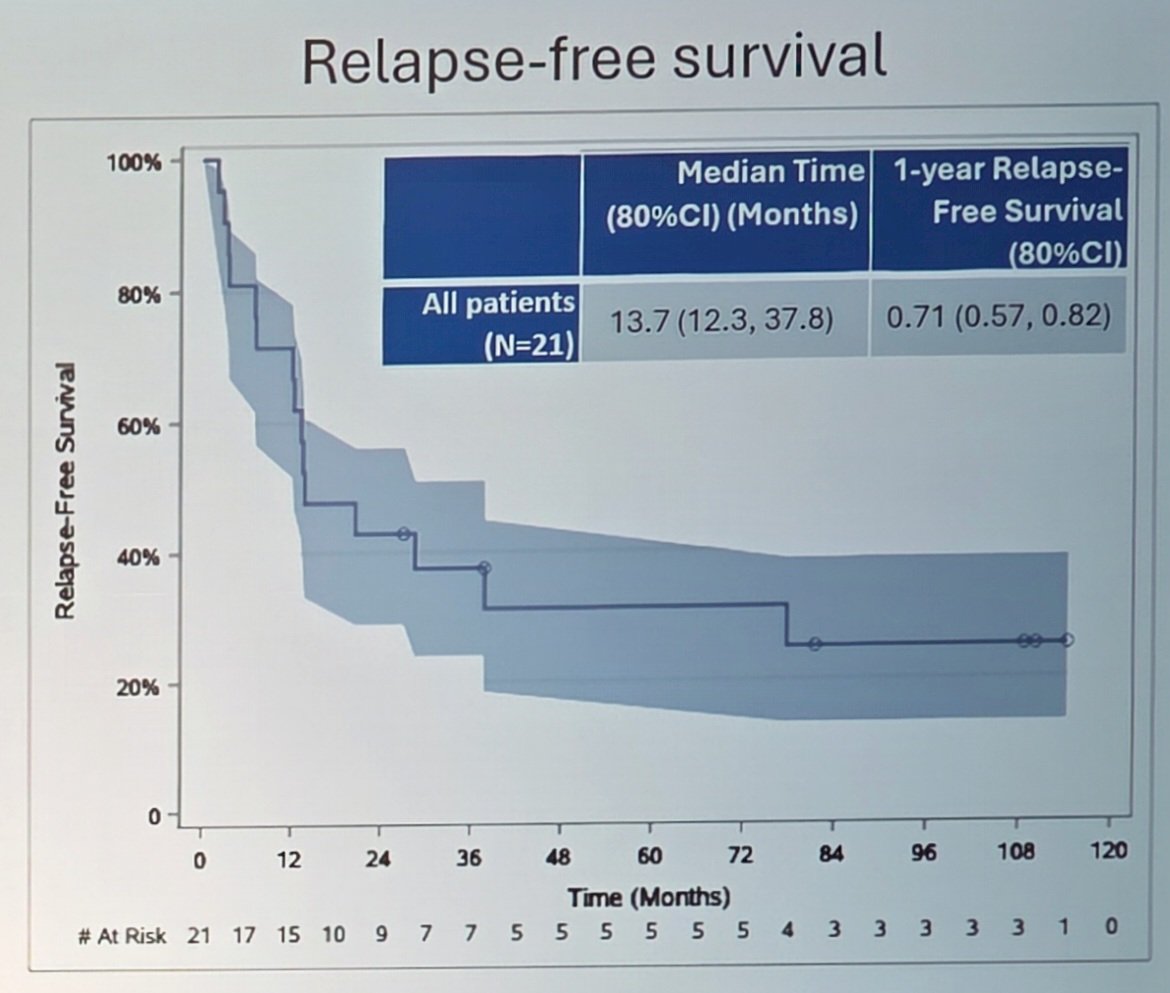
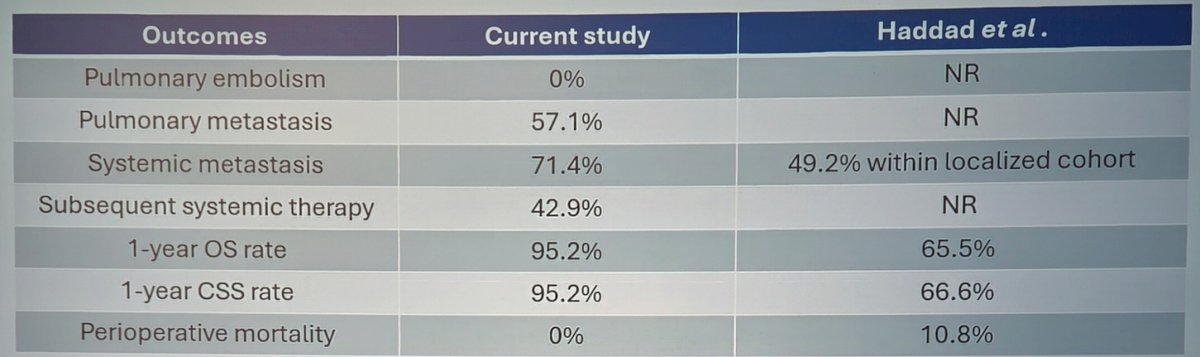
This was based on a prespecified primary efficacy endpoint historically for surgery of 55.7% 1-year relapse-free survival, with an expected increase of 16.7% with neoadjuvant stereotactic ablative body radiotherapy to the IVC tumor thrombus. The trial met the prespecified phase II primary efficacy endpoint, with 1-year relapse-free survival significantly exceeding the historical surgery alone benchmark. The following table highlights the secondary outcomes compared to a historical control:
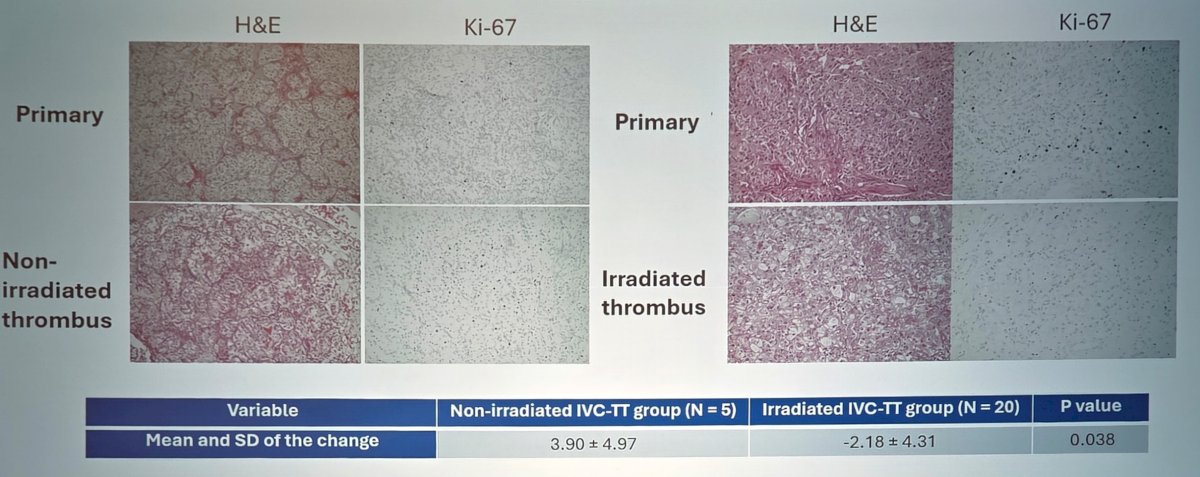
There were no radiation-related grade 4+ adverse events, and 36.4% of patients had a perioperative grade 3+ adverse event. From a correlative perspective, Dr. Lin and colleagues found that neoadjuvant stereotactic ablative body radiotherapy to the IVC tumor thrombus reduced Ki-67 expression in the tumor sample:
Dr. Lin concluded this presentation discussing a phase II trial of neoadjuvant stereotactic ablative radiotherapy for caval thrombus in newly diagnosed RCC with the following take-home points:
- Neoadjuvant stereotactic ablative body radiotherapy followed by surgery is a feasible and safe approach for RCC with IVC tumor thrombus
- The trial met its prespecified phase II primary endpoint, with 1-year relapse-free survival significantly exceeding the historical surgery alone benchmark
- These results demonstrate promising oncologic efficacy with limited toxicity and support further evaluation of neoadjuvant stereotactic ablative body radiotherapy in this high-risk RCC population
Presented by: Lin Lin, MD, Division of Urology, UT Southwestern, Dallas, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.