(UroToday.com) The 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix between December 2 and December 5, 2025, was host to the Poster Session. Dr. Can Aydogdu presented poster # 203: Role of ctDNA testing in BCG-exposed non-muscle-invasive bladder cancer: a real-world analysis.
Dr. Aydogdu opened his presentation by noting that patients with non–muscle-invasive bladder cancer (NMIBC) who do not respond to intravesical Bacillus Calmette-Guérin (BCG) therapy face the highest risk of disease progression. He noted that radical cystectomy remains the current gold standard for these BCG-unresponsive cases. Although several novel intravesical agents have emerged in recent years with the goal of sparing the bladder. However, a considerable proportion of patients who ultimately undergo radical cystectomy are found to be upstaged on final pathology. This underscores the frequent clinical understaging in NMIBC and the potential undertreatment of patients managed exclusively with intravesical therapy.
Dr Aydogdu’s team evaluated a cohort of patients with BCG-exposed NMIBC and analyzed their circulating tumor DNA (ctDNA) profiles to assess the role of ctDNA surveillance in improving disease detection and staging accuracy.
The investigators conducted a retrospective review of NMIBC patients with prior BCG exposure categorized as BCG-unresponsive, recent BCG, or remote BCG according to AUA/SUO guideline definitions. (1) All patients underwent serial ctDNA testing using a personalized, tumor-informed assay (Signatera, Natera), with samples collected at baseline and then every 3 months. ctDNA positivity was defined as the detection of ≥2 tumor-specific variants.
Baseline clinical stage, ctDNA findings, and staging from subsequent cross-sectional imaging and/or cystoscopy performed during routine care were evaluated to identify both clinical upstaging (≥cT2 or cN+ on imaging) and pathologic upstaging (higher pathologic stage or nodal involvement at radical cystectomy compared with the initial clinical stage).
Dr. Aydogdu highlighted that a total of 17 BCG-exposed patients (median age 70 years [IQR 67–73]; 88% male; 88% pure urothelial histology) underwent ctDNA surveillance: 10 were BCG-unresponsive, 3 had recent BCG, and 4 had remote BCG exposure. At presentation, 14 patients (82%) had cT1 disease, 2 (12%) had cTis, and 1 (6%) had cTa. Concomitant CIS was identified in 7 patients (47%). Following imaging, 13 patients (76%) remained cTa/cTis/cT1, whereas 4 (24%) were clinically upstaged to ≥cT3.
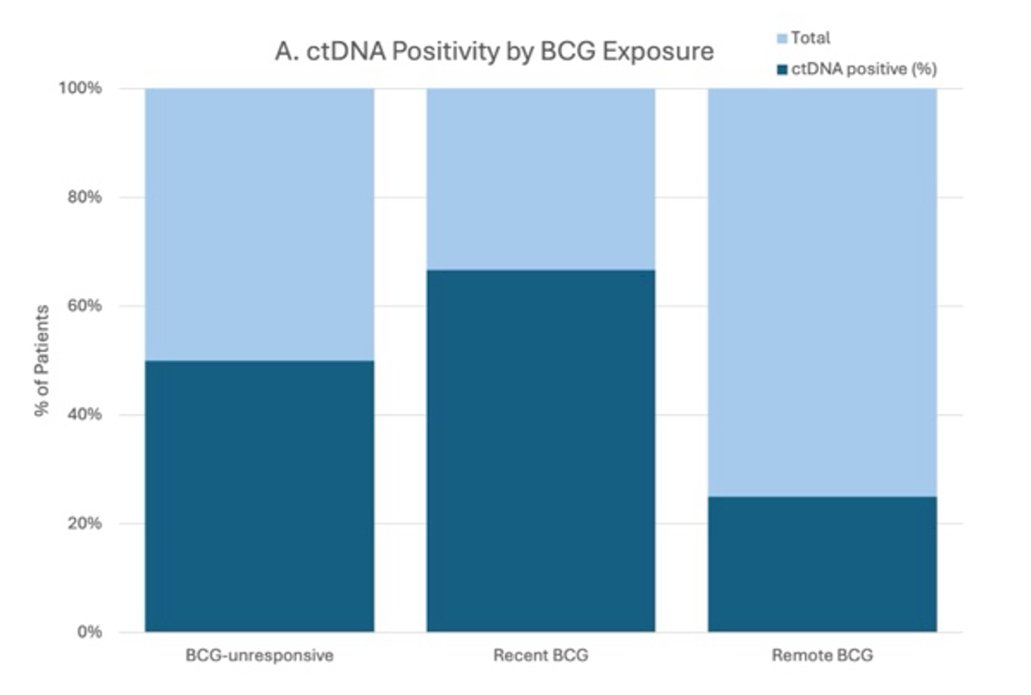
Dr. Aydogdu further highlighted that ctDNA positivity was detected in 8/17 patients (47%), with notable variation by BCG exposure:
- 5/10 (50%) in BCG-unresponsive
- 2/3 (66%) in recent BCG
- 1/4 (25%) in remote BCG (as illustrated below)
When stratified by clinical stage:
- 5/13 (38%) of Ta/Tis/T1 patients were ctDNA-positive
- 3/4 (75%) of ≥cT3 cases were ctDNA-positive
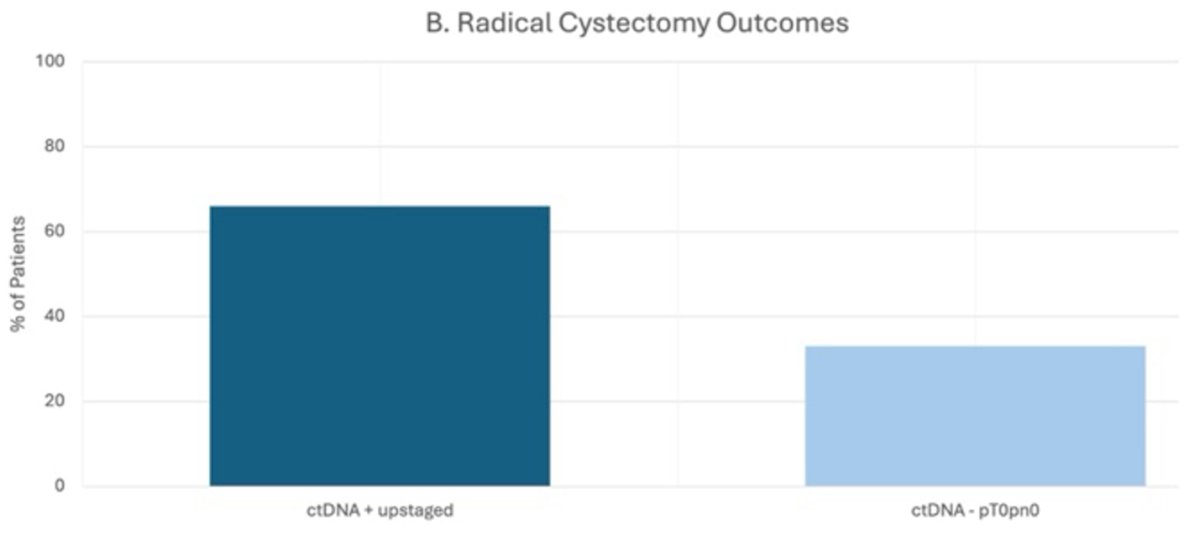
Moreover, 6 patients proceeded to radical cystectomy. Among the 4 patients with positive ctDNA, all were pathologically upstaged, with final pathology showing pT1 + Tis pN0, pT2b pN0, pT1 pN2, and pT3a pN1. In contrast, the 2 ctDNA-negative patients had no residual tumor in the surgical specimen (pT0 pN0) as illustrated in the figure below.
Dr. Aydogdu concluded the presentation of their poster with the following remarks:
- ctDNA positivity was more common in patients with locally advanced disease and was detected in over half of those who proceeded to radical cystectomy, all of whom were pathologically upstaged.
- All patients with pT0 pN0 pathology at cystectomy were ctDNA-negative.
- ctDNA positivity was also identified in a subset of clinically staged cT1 cases, suggesting occult extravesical disease not captured by conventional staging.
- These findings raise concern for potential undertreatment when relying solely on intravesical therapy in selected patients.
- Overall, the results highlight the potential value of ctDNA surveillance in refining risk stratification and identifying patients who may benefit from earlier definitive treatment.
Presented by: Can Aydogdu, MD, Department of Urology, Klinikum der Universität München, Munich, Germany
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Penn State Health, Hershey, PA. United States of America @chavarriagaj on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References: