(UroToday.com) The 2025 Society of Urologic Oncology (SUO) annual meeting, held in Phoenix between December 2 and December 5, 2025, was host to the Poster Session. Dr. Jethro Kwong presented poster #199: RECURxNCE-BCa – an artificial intelligence-based tool to predict recurrence in non-muscle invasive bladder cancer and comparison with current risk stratification tools for intermediate-risk disease.
Dr. Kwong highlighted that accurate prognostication of tumor recurrence in patients with non–muscle invasive bladder cancer (NMIBC) is critical for optimizing patient counselling and guiding management decisions. However, existing nomograms used to predict recurrence risk are limited, as they do not fully reflect current clinical practices or contemporary treatment patterns, resulting in suboptimal performance and reduced applicability in modern NMIBC care.
The investigators hypothesized that their artificial intelligence (AI)–based model, RECURxNCE-BCa (RECURrence risk assessment in non-muscle invasive bladder cancer), would outperform existing prediction tools by providing more accurate, contemporary, and individualized recurrence risk estimates for NMIBC patients.
This study was performed within the STREAM-URO collaborative framework and included a large multinational dataset. The training cohort comprised 3,797 NMIBC patients treated across 34 North American and European centers between January 1, 2005, and December 31, 2023, while an independent held-out validation cohort included 8,862 patients from the same institutions and time period.
The primary outcome was time to recurrence, defined as the first tumour event during follow-up. RECURxNCE-BCa was developed using a random survival forest model trained on 14 routinely collected clinicopathologic variables. Its performance was benchmarked against established tools, including the EORTC and CUETO nomograms, the EORTC 2016 and EAU risk-group systems, as well as a LASSO Cox model built using the same feature set as RECURxNCE-BCa.
The model was evaluated using several complementary performance metrics, including the concordance index to assess discriminative accuracy, smoothed calibration plots to examine agreement between predicted and observed recurrence risk, and decision-curve–based net benefit to determine clinical utility. The investigators also quantified bias by comparing differences in c-index between RECURxNCE-BCa and all baseline models across multiple patient subgroups. Finally, the model’s ability to refine intermediate-risk NMIBC was tested using three approaches: RECURxNCE-BCa–derived risk estimates, the International Bladder Cancer Group (IBCG) risk-factor system, and a simplified low vs high-risk schema in which high risk was defined by either multifocal disease or tumour size >3 cm.
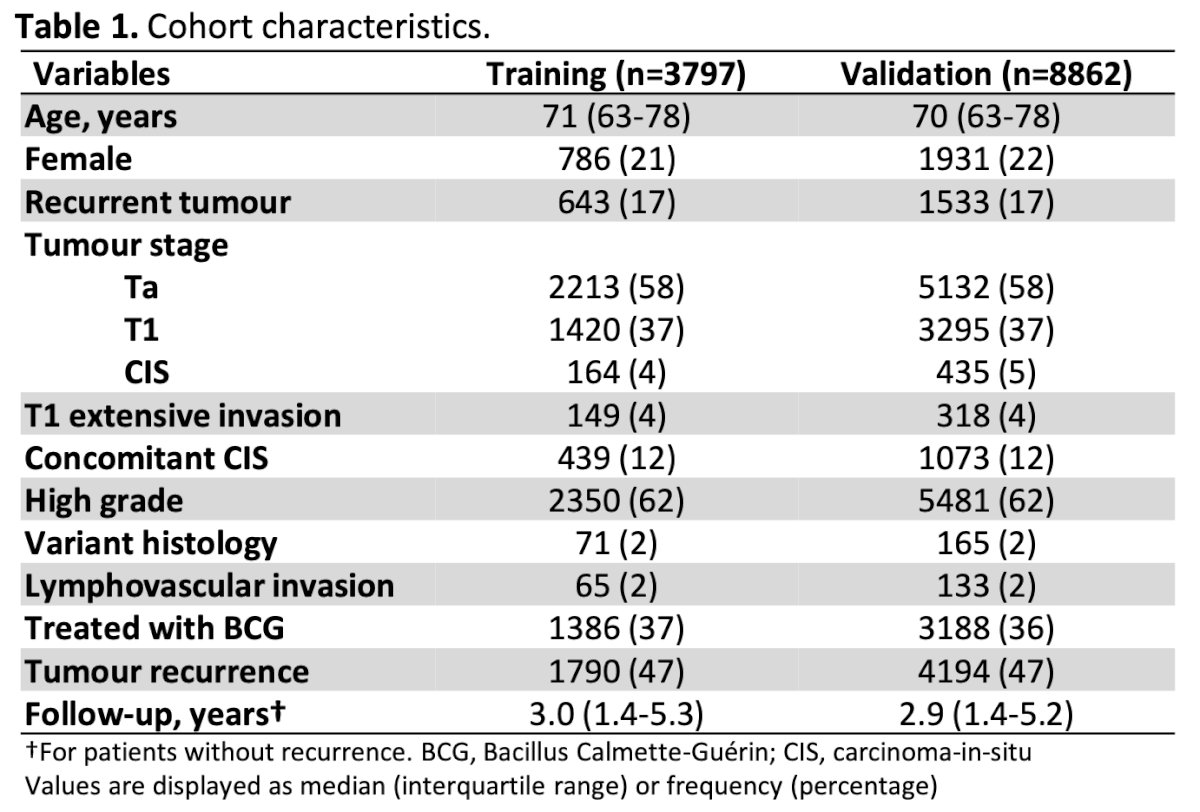
Dr. Kwong noted that cohort characteristics were well balanced between the training (n=3,797) and validation (n=8,862) sets. Most patients in both cohorts had Ta tumors (58%), while only a small proportion had CIS (4% and 5%, respectively). High-grade disease was predominant, occurring in 62% of patients in each cohort. Median follow-up was similar across groups 3.0 years in the training cohort and 2.9 years in the validation cohort.
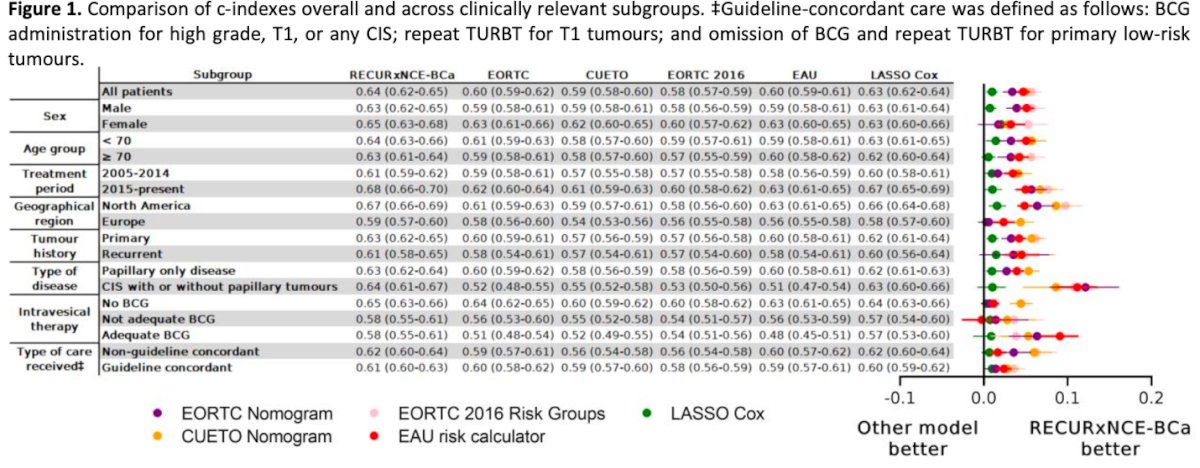
Dr. Kwong highlighted that RECURxNCE-BCa consistently outperformed all benchmark models across nearly every clinically relevant subgroup. In the overall cohort, the model achieved the highest concordance index, with clear separation favoring RECURxNCE-BCa compared to the EORTC and CUETO nomograms, the 2016 EORTC risk groups, the EAU risk calculator, and the LASSO Cox model. This performance advantage was preserved in both men and women, in patients younger and older than 70 years, and across treatment eras (2005–2014 and 2015–present), as illustrated in the figure below.
Importantly, RECURxNCE-BCa maintained superior discrimination in key high-risk subgroups, including patients with recurrent tumors, CIS, high-grade disease, and those who did not receive adequate BCG. Even among patients who received guideline-concordant management, RECURxNCE-BCa remained the highest-performing model, highlighting its robustness across heterogeneous clinical contexts. Overall, the figure demonstrates a consistent rightward shift of RECURxNCE-BCa compared with all comparators, underscoring its stronger predictive accuracy for tumor recurrence in NMIBC.
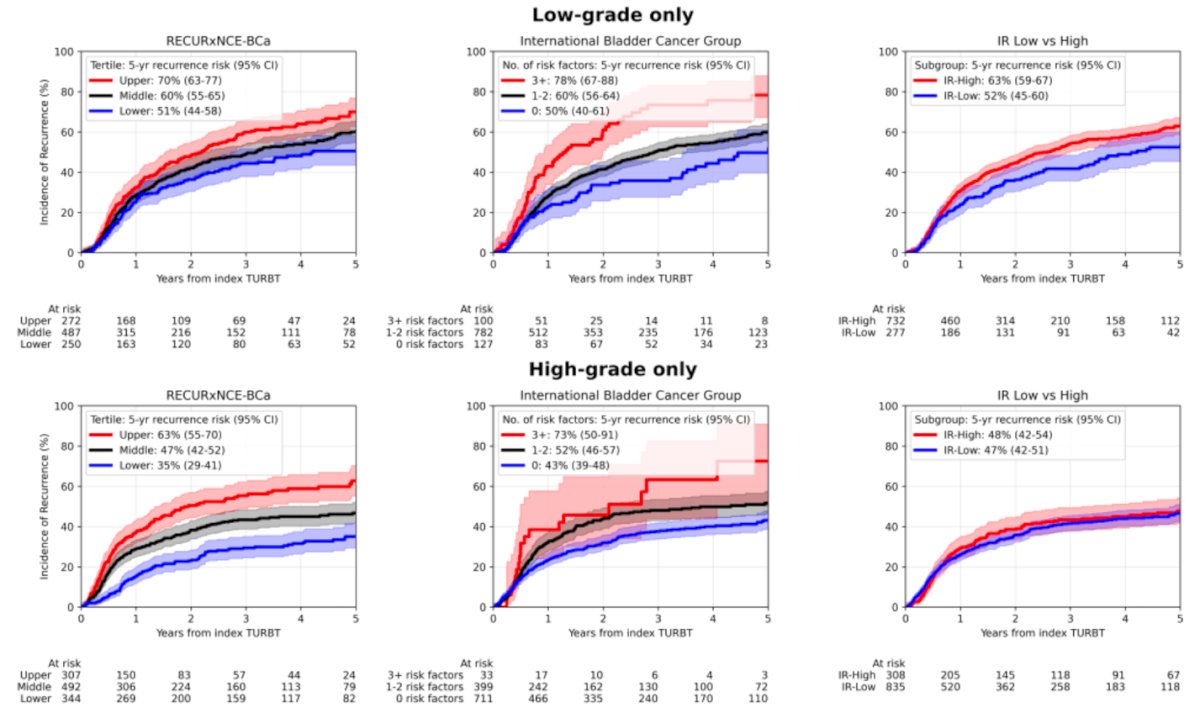
Notably, the investigators demonstrated that RECURxNCE-BCa provides a more meaningful sub-stratification of intermediate-risk NMIBC compared to existing systems, with clearer separation of recurrence trajectories over five years. Using tertiles, RECURxNCE-BCa distinguishes three clinically relevant risk groups whose recurrence curves diverge early and remain well separated in both low-grade and high-grade cohorts. Five-year recurrence estimates ranged from 51% to 70% in low-grade cases and from 35% to 63% in high-grade cases, showing tighter calibration and more granular risk discrimination.
When compared with the IBCG risk-factor system, RECURxNCE-BCa demonstrated greater separation between groups, particularly in the high-grade cohort, where IBCG categories overlapped more prominently. Similarly, the simplified IR Low vs High system produced only a modest distinction between curves, especially in high-grade disease, where both groups showed nearly identical five-year recurrence risks. Overall, these plots highlight the superior ability of RECURxNCE-BCa to refine risk stratification within the clinically challenging intermediate-risk NMIBC population, capturing meaningful heterogeneity that traditional systems fail to resolve.
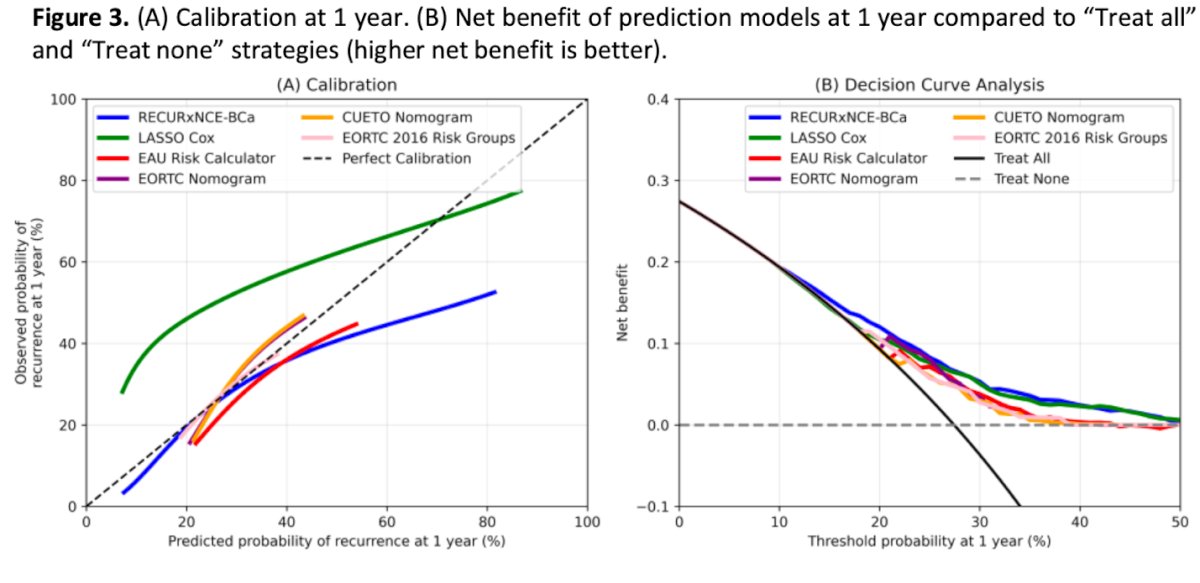
RECURxNCE-BCa showed markedly better calibration at one year, with predicted recurrence risk closely aligning with observed outcomes, while traditional tools such as EORTC, CUETO, and the EAU calculator consistently underestimated risk across the spectrum. Decision curve analysis demonstrated that RECURxNCE-BCa provided the highest net clinical benefit across a wide range of threshold probabilities, outperforming all comparator models and offering clearer utility over “treat all” or “treat none” strategies as illustrated below.
Dr. Kwong concluded his poster presentation with the following take home messages:
- RECURxNCE-BCa outperformed all existing risk tools for predicting recurrence in the largest NMIBC cohort ever evaluated.
- Despite superior performance, overall accuracy remains modest, likely reflecting real-world variability in surgical quality, perioperative care, and other unmeasured clinical factors.
- In intermediate-risk NMIBC, RECURxNCE-BCa substratification performed comparably to the IBCG system while providing a more balanced distribution of patients across risk tertiles.
Presented by: Jethro Kwong, MD, MSc, Resident Physician, Division of Urology, University of Toronto, Toronto, ON
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Penn State Health, @chavarriagaj on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.