(UroToday.com) The 2025 SUO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Can Aydogdu discussing the genomic drivers of ctDNA detection and their prognostic impact in muscle invasive bladder cancer. Among muscle invasive bladder cancer patients, 30-50% will relapse after curative therapy. ctDNA is a promising biomarker for recurrence detection among muscle invasive bladder cancer, but its sensitivity varies. Higher T and N stage predict ctDNA positivity, reflecting greater tumor burden and shedding. The influence of specific tumor genomic alterations on ctDNA detection is less understood in muscle invasive bladder cancer. Thus, identifying genomic predictors of ctDNA positivity could refine surveillance strategies, improve interpretation of negative results, and better integrate ctDNA into post-treatment monitoring.
Dr. Aydogdu and colleagues retrospectively identified patients with muscle invasive bladder cancer treated with curative intent (neoadjuvant chemotherapy + radical cystectomy, radical cystectomy alone, or bladder-preserving therapy) between 2022 and 2025. Tumor tissue underwent targeted next-generation sequencing (Altera platform). Actionable mutations were defined as alterations in FGFR3, FGFR2, ERBB2, PIK3CA, HRAS, MSH2, MSH6, MLH1, or PMS2. Serial ctDNA testing (up to 11 posttreatment draws) was performed using the Signatera assay (Natera, Inc.) and classified as positive or negative per draw. ctDNA/tissue concordance was defined as ≥1 actionable tumor mutation with ctDNA positivity at any time, tissue unique as ≥1 actionable mutation without ctDNA positivity, ctDNA unique as ctDNA positivity without an actionable mutation, and no actionable as absence of both. Analyses were conducted in Python, including Fisher’s exact tests for gene enrichment in ctDNA-positive patients and oncoprint visualization. Recurrence free survival by presurgical ctDNA status was assessed using Kaplan–Meier methods.
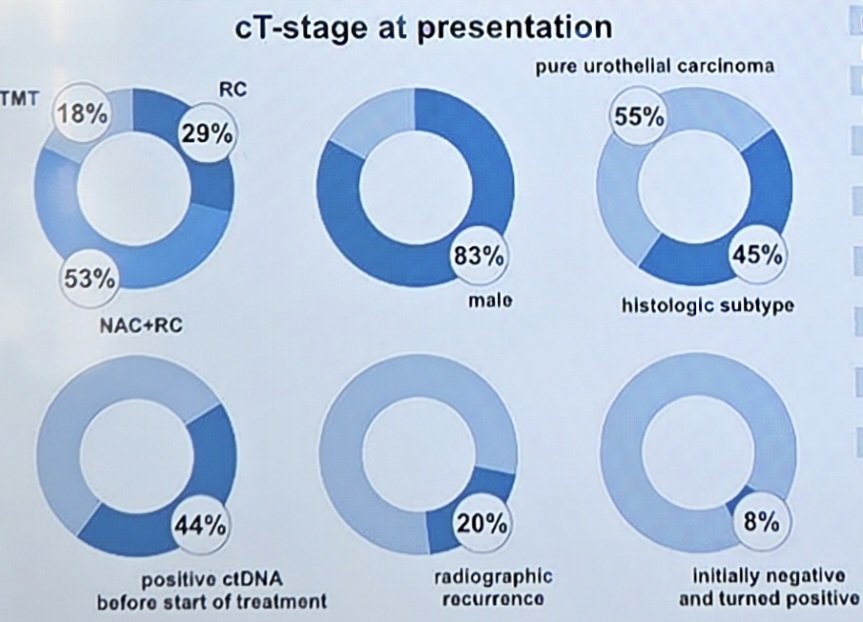
There were 66 patients with a median age of 69.5 years (IQR 61–73) that underwent curative-intent treatment, including neoadjuvant chemotherapy + radical cystectomy (53%), radical cystectomy alone (29%), and bladder-preserving therapy (18%), with available data. Overall, 83% were male, 55% had a pure urothelial carcinoma subtype, and 44% had a positive ctDNA before the start of treatment:
Across the cohort, ctDNA/tissue concordance was observed in 18.9% of patients, while 34.0% harbored tissue-unique mutations, 26.4% had ctDNA-unique mutations, and 20.8% had no detectable actionable mutations. Among patients who initially had a negative ctDNA, 92% remained negative.
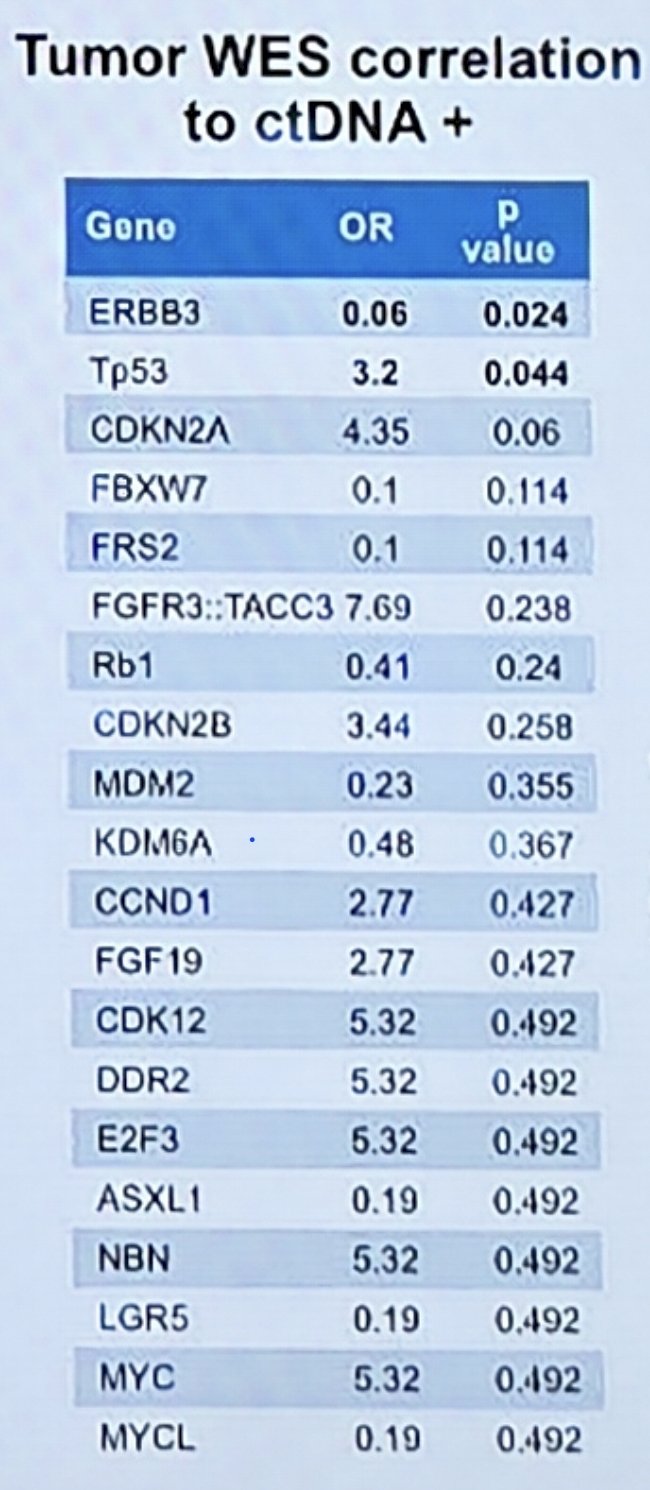
The highest concordance rate occurred in patients with an intermediate ctDNA burden (1.0–2.5 MTM/mL), where 67% demonstrated concordant ctDNA profiles. Among ctDNA-positive patients, CDKN2A (OR 4.35, p = 0.06) was among the most enriched genes:
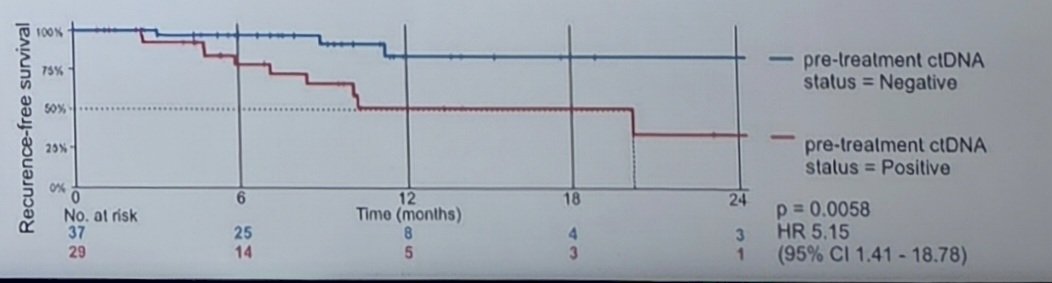
Overall, presurgical ctDNA positivity was strongly associated with worse recurrence free survival, while ctDNA-negative patients showed durable disease control (HR 5.15, 95% CI 1.41-18.78; log-rank p = 0.067):
Dr. Aydogdu concluded this presentation discussing the genomic drivers of ctDNA detection and their prognostic impact in muscle invasive bladder cancer with the following take home points:
- Certain genomic alterations may be associated with ctDNA positivity in muscle invasive bladder cancer and could help refine surveillance
- Initial negative ctDNA remained negative in most cases and suggesting further exploration of neoadjuvant de-escalation
Presented by: Can D. Aydogdu, MD, LMU University Hospital, Munich, Germany; Cleveland Clinic Foundation, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.