(UroToday.com) The SUO 2025 Annual Meeting featured a poster presentation by Dr. Mark Tyson reporting preliminary findings from Cohort A of the ADVANCED-2 trial, an ongoing phase II, open-label trial evaluating TARA-002, a novel intravesical immunopotentiator, in BCG-naïve high-grade NMIBC.
Current standard treatment relies heavily on BCG, yet access challenges and variable efficacy highlight the need for additional bladder-sparing options.1,2 TARA-002 is a TLR2/NOD2 agonist derived from inactivated Streptococcus pyogenes, designed to activate innate and adaptive immune responses and previously shown to be safe with evidence of antitumor activity in BCG-unresponsive NMIBC.3,4
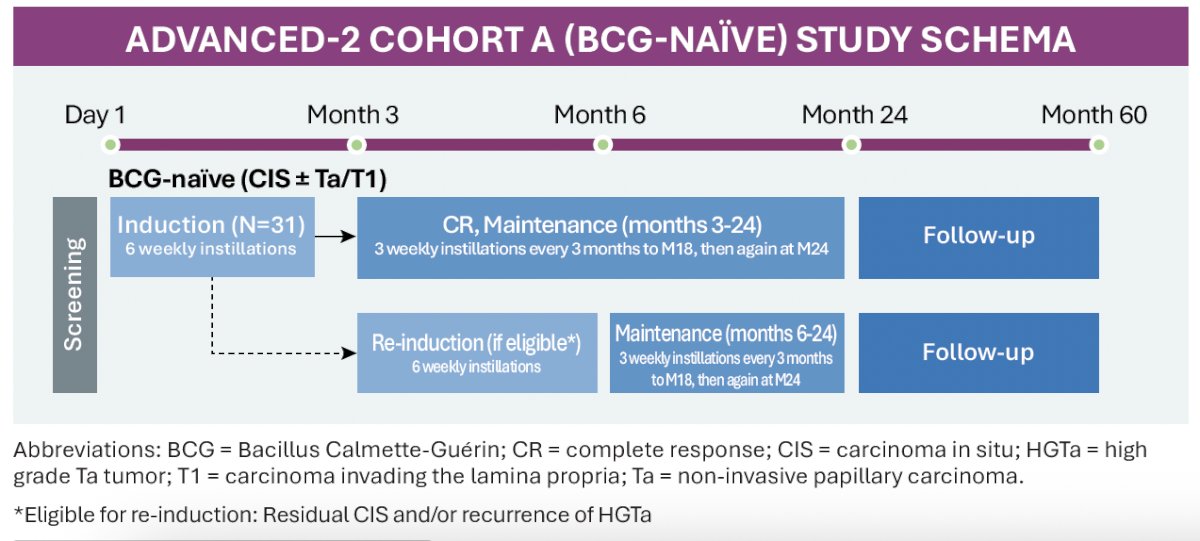
ADVANCED-2 (NCT05951179) is a phase II, ongoing, open-label study enrolling adults 18 years or older with high-grade NMIBC with CIS ± Ta/T1 who are BCG-naïve, defined as no prior BCG exposure or more than 24 months since last BCG administration. The primary endpoint is high-grade complete response (CR) at any time, assessed by central pathology. The key secondary endpoints include duration of response through 12 months. The data cutoff date was November 7, 2025.
Treatment consisted of a 6-week induction course followed by 3-week maintenance cycles every 3 months through Month 18, and again at Month 24. Participants with residual CIS or recurrent HG Ta were eligible for a 6-week re-induction course, followed by resumed maintenance.
Thirty-one BCG-naïve participants were included in this preliminary analysis. The median age was 71 years (range 45–89); 80.6% were male, and 93.5% were White.
Efficacy
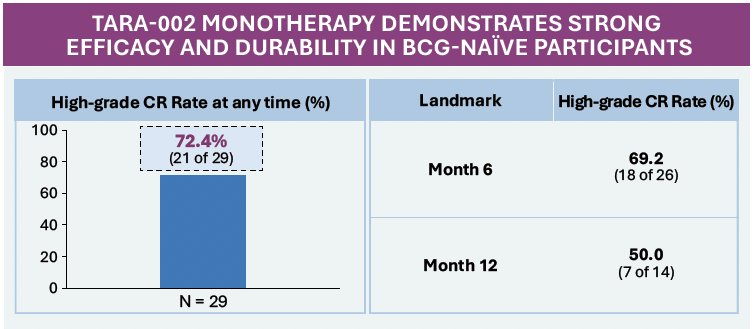
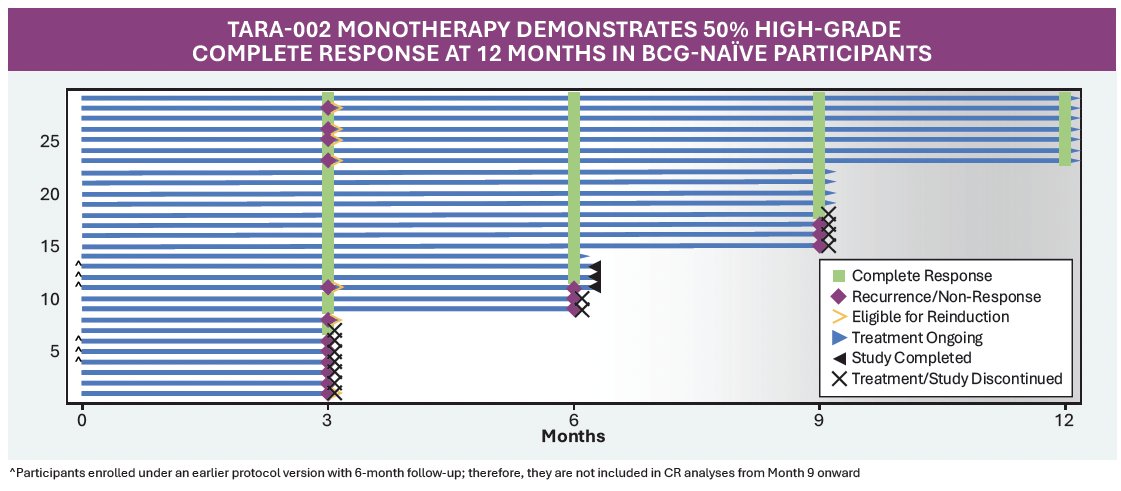
Among 29 evaluable participants, the high-grade CR rate at any time was 72.4% (21/29). Landmark CR rates were 69.2% at Month 6 (18/26) and 50% at Month 12 (7/14).
The response durability among initial responders was encouraging: 87.5% (14/16) maintained their CR at Month 6, and all evaluable responders (3/3) maintained CR through Month 12.
Re-induction appeared active in initial non-responders: 80% (4/5) achieved a CR by Month 6 following re-induction, with all maintaining CR through the Month 12 assessment (4/4).
Safety
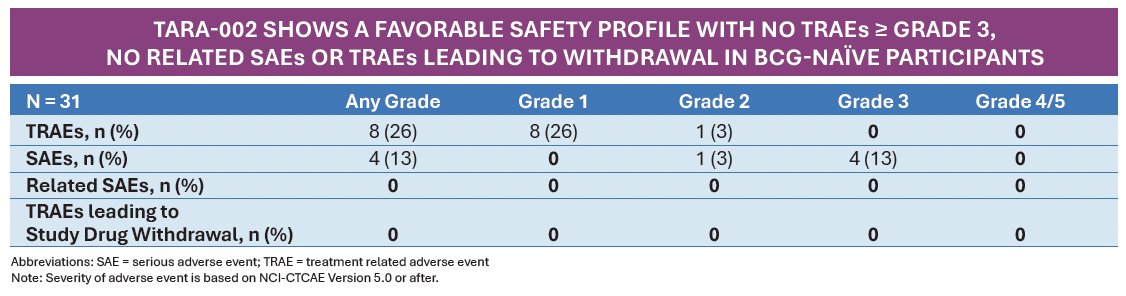
TARA-002 was well tolerated, with a favorable safety profile. Treatment-related adverse events (TRAEs) occurred in 26% of participants (8/31), all Grade 1 except one Grade 2 event; no Grade 3 or higher TRAEs were reported. No treatment-related serious adverse events occurred. Reported TRAEs were primarily mild urinary symptoms such as dysuria, hematuria, and fatigue, consistent with the expected intravesical therapy profile.
Dr. Tyson concluded as follows:
- In BCG-naïve high-grade NMIBC participants, TARA-002 demonstrated a high rate of complete response with a substantial proportion maintaining a durable response at 1 year
- Re-induction therapy successfully salvaged most initial non-responders, resulting in high conversion rates and durable responses
- TARA-002 was well tolerated; common urinary TEAEs reflect urinary tract instrumentation effects and systemic TEAEs were mild and easily managed
- These findings support continued investigation of TARA-002 in BCG-naïve HG-NMIBC
Presented by: Mark Tyson, MD, MPH, Associate Professor, Department of Urology, Mayo Clinic, Phoenix, AZ
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References:
- Chang SS, Boorjian SA, Chou R, et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline. J Urol. 2020;203:1122–1134.
- Kamat AM, Flaig TW, Grossman HB, et al. Definitions, end points, and clinical trial designs for BCG-unresponsive NMIBC. J Clin Oncol. 2016;34:1935–1944.
- Steinberg RL, Thomas LJ, O’Donnell MA, et al. Intravesical therapy for NMIBC: Current landscape and future directions. Eur Urol Focus. 2022;8:20–29.
- Shore ND, Cookson MS, Gomella LG, et al. Contemporary management patterns for high-risk NMIBC in the United States. Urol Pract. 2024;11:185–194.