(UroToday.com) At the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Dr. Roger addressed the rapidly evolving role of urinary tumor DNA (utDNA) for minimal residual disease (MRD) detection in non–muscle-invasive bladder cancer (NMIBC). His talk centered on a fundamental clinical need: identifying biologically meaningful disease recurrence early enough to influence treatment strategy, while avoiding overtreatment in patients unlikely to recur.
Dr. Li framed the discussion around two distinct, MRD-relevant clinical objectives in NMIBC:
- In low-risk NMIBC: Improving risk stratification to potentially reduce the frequency of surveillance cystoscopies
- In high-risk NMIBC: Enabling early recurrence detection to inform timely escalation of therapy—a setting in which high positive predictive value (PPV) is essential for clinical utility.
Why have so many urinary biomarkers failed? This challenge has persisted for decades: despite wide interest, urine-based biomarkers have yet to meaningfully alter NMIBC surveillance paradigms. Reasons for these historical shortcomings include:
- Tumor heterogeneity, including multifocality and field cancerization
- Background genomic noise from inflammation or benign urothelial shedding
- Low sensitivity for flat lesions and CIS
- Poor positive predictive value (PPV), especially in surveillance intervals with low prevalence
- Temporal discordance between biologic activity and endoscopic detectability
The images below highlight the challenges in achieving a high PPV: small, subtle, or flat lesions often escape detection, while multifocal recurrences may be missed until they become visually apparent. This underscores the unmet need for a biomarker capable of capturing biologic recurrence, not merely visible tumor.
Dr. Li reviewed contemporary urine tests—protein-based, methylation-based, and next-generation sequencing assays. Most share one common trend: acceptable sensitivity and specificity, but insufficient PPV.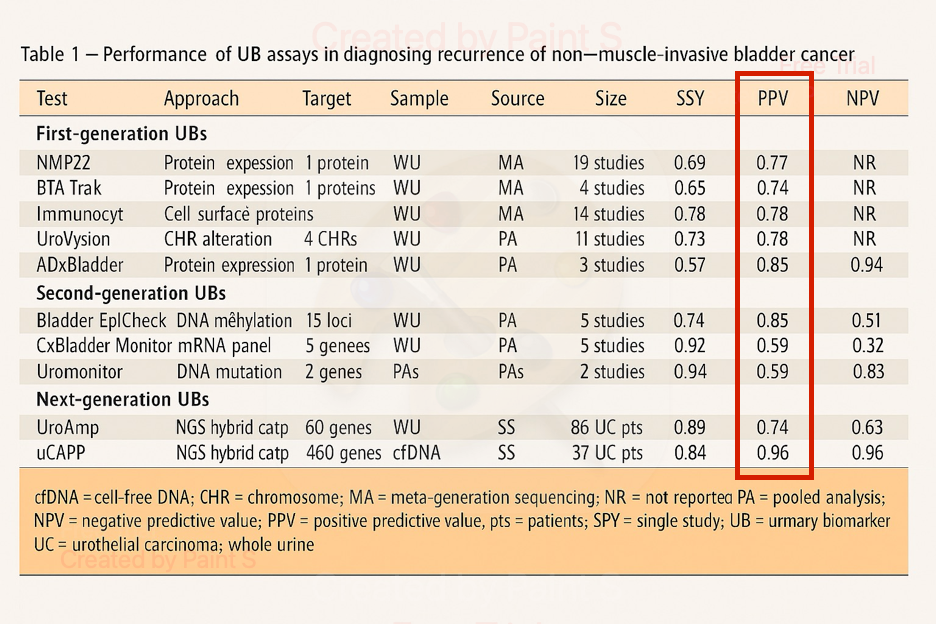
Even next-generation assays, such as epigenetic panels and fixed-gene NGS panels, have been unable to deliver PPV levels high enough to justify treatment escalation. While some assays demonstrate robust sensitivity, many falsely identify patients as “at risk,” producing clinical uncertainty and limiting adoption.
Validation data presented reinforced this pattern: across multiple assays, including those leveraging NGS, PPV rarely reaches the reliability threshold needed for high-risk NMIBC decision-making.
Urothelial carcinogenesis proceeds through a continuum—normal urothelium → dysplasia → CIS → invasive carcinoma. During this process, many non-malignant or pre-malignant cells may shed into urine, carrying genomic alterations that mimic tumor-associated signals.
Thus, not all DNA in urine is tumor-derived. This “background noise” dilutes the interpretability of fixed-panel mutation assays, where any detected mutation is presumed malignant—even when it may represent benign clonal expansion.
This challenge—unique to bladder cancer—means that achieving high PPV requires a strategy that can discriminate true tumor-derived mutations from background genomic drift.
Transition to utDNA MRD: A Personalized, Tumor-Informed Solution
Tumor-informed MRD detection represents a paradigm shift already transforming other cancers (e.g., colorectal, lung). The utDNA workflow adapts this approach to urine, generating a personalized mutation panel derived from each patient’s index tumor.
The utDNA MRD workflow is as follows:
- Index TURBT undergoes whole-exome sequencing.
- Patient-specific mutations are selected to create a personalized hybrid-capture panel.
- Pre- and post-surgical urine samples are analyzed for these exact mutations.
- Any detection of these mutations in urine represents true tumor-derived DNA, enabling highly specific MRD assessment.
Because only tumor-specific mutations are queried, background noise drops dramatically, improving PPV. Unlike fixed-gene panels, this approach does not assume that the same mutation is always pathogenic—it is pathogenic only if it came from that patient’s tumor.
Dr. Li transitioned to discussing a study from his group evaluating the utility of utDNA for detecting MRD following a TURBT. The baseline characteristics are summarized below:
He noted that the mutational burden of index TURBT tumors was consistent with typical NMIBC genomic profiles. Importantly, most tumor-derived mutations were traceable in urine, supporting the feasibility of tumor-informed urine MRD testing.
The mutational landscape heatmap demonstrated a robust biological signal, enabling confident mutation tracking in the downstream analysis.
The performance metrics for utDNA for detecting MRD were remarkable:
- AUC = 0.932, indicating excellent overall accuracy.
- Tumor fraction and composite mutation scores were markedly higher in MRD-positive cases, with clear separation from MRD-negative samples.
- Scatterplots illustrated that even low-level MRD-positive cases demonstrated detectable, patient-specific tumor mutations—supporting the sensitivity and robustness of the assay.
Dr. Li emphasized that this degree of accuracy has not been observed with fixed-panel biomarker tests and supports the biological validity of the tumor-informed approach.
The table below highlights examples of “private” mutations—genomic alterations present in a patient’s tumor but not represented in standard diagnostic panels. utDNA MRD was able to detect these private mutations in urine, demonstrating a major advantage over conventional assays: utDNA MRD does not depend on a universal panel—it depends on your tumor. This flexibility is essential in bladder cancer, where no single gene or mutation dominates across patients.
Clinical Utility: Longitudinal Monitoring and Early Recurrence Detection
Dr. Li concluded by showing longitudinal utDNA heatmaps, which tell a biologically compelling story:
- In patients who experience NMIBC recurrences, utDNA signals often become positive before or at the time of visual detection.
- In patients with no recurrence, utDNA remained persistently negative or low-level.
- utDNA trajectories mirrored tumor biology more consistently than cystoscopic timing.
This provides a strong rationale for utDNA MRD as a surveillance adjunct, particularly in high-risk NMIBC, where early recurrence detection is crucial.
Dr. Li highlighted several key take-home messages:
- High PPV is the critical requirement for any biomarker that might influence treatment escalation.
- NGS-based utDNA is uniquely capable of meeting this requirement by capturing comprehensive, patient-specific molecular information.
- Tumor-informed utDNA MRD appears to outperform other urinary biomarkers in biologic specificity and predictive accuracy.
- Future research will focus on longitudinal validation, prognostic modeling, and integration into risk-adapted NMIBC management strategies.
- utDNA MRD detection represents one of the most promising advances toward biologically guided NMIBC surveillance and treatment intensification.
Presented by: Roger Li, MD, Genitourinary Oncologist, Moffitt Cancer Center, Tampa, FL
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
Related content: Urine Tumor DNA as a Biomarker for High-Risk Bladder Cancer Recurrence and Guidance - Roger Li