(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a bladder cancer poster session. Dr. Ahmet Yildirim presented a study evaluating how neuropathy guides clinical decision-making and predicts survival in 1st line enfortumab vedotin + pembrolizumab (EV+P) for metastatic urothelial carcinoma (mUC).
EV+P is currently the standard-of-care, first-line regimen for locally advanced or mUC, based on the results of EV-302.1 Its use is complicated by peripheral neuropathy, which often requires dose interruptions. Clinicians must frequently balance the requirement to manage worsening peripheral neuropathy against the risk of losing treatment efficacy. The study investigators evaluated whether holding treatment for toxicity impacts survival outcomes in a real-world cohort.
The study investigators retrospectively analyzed 41 patients treated with first-line EV+P at the Winship Cancer Institute of Emory University. Survival outcomes were estimated using Kaplan-Meier methods and Cox regression analyses to assess the impact of dose interruptions on survival.
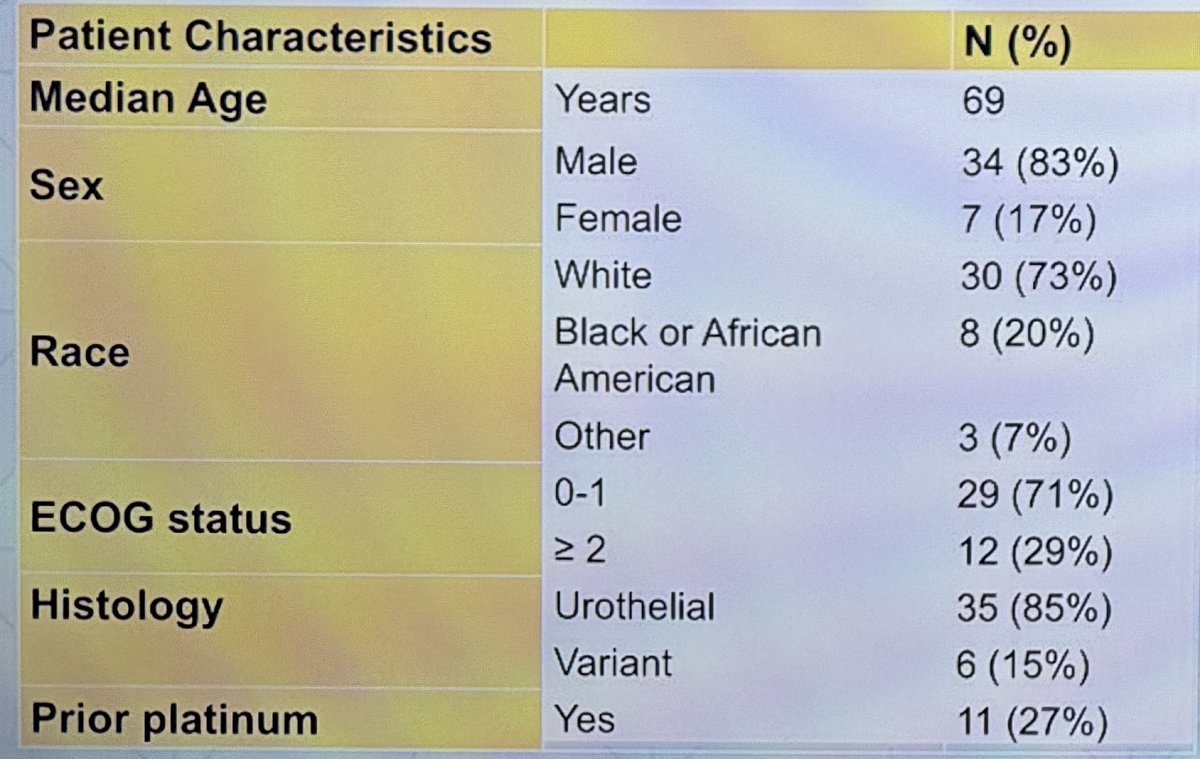
The key baseline patient characteristics are as follows:
- Median age: 69
- Male: 34 (83%)
- Race: White 30 (73%), Black/African American 8 (20%), Other 3 (7%)
- ECOG 0–1 in 29 (71%); ECOG ≥2 in 12 (29%)
- Histology: Urothelial 35 (85%), Variant 6 (15%)
- Prior platinum: 11 (27%)
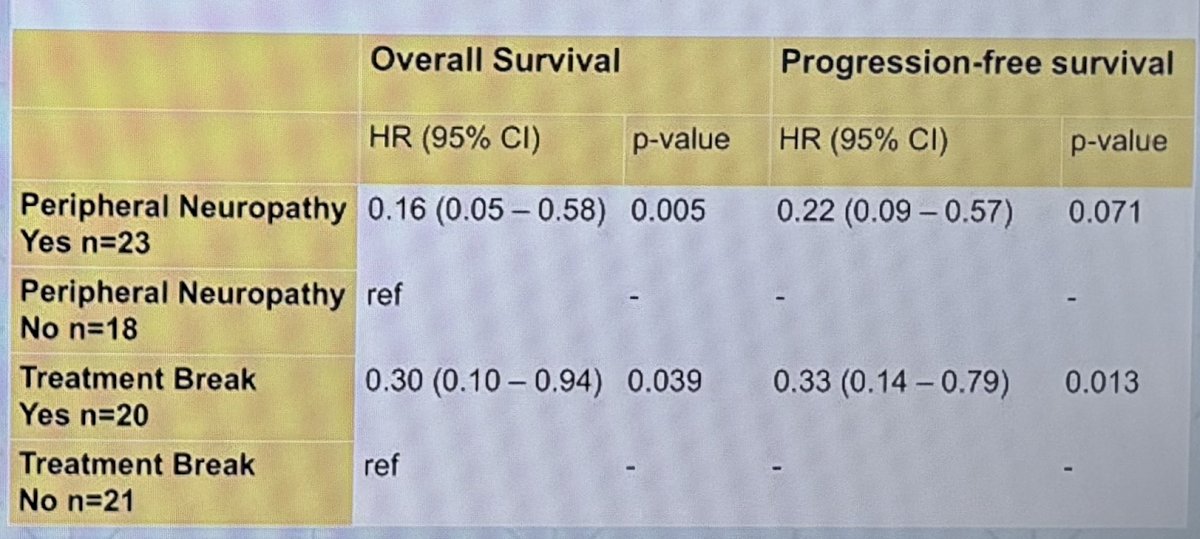
Among the 41 patients treated with first-line EV+P, the development of treatment-emergent peripheral neuropathy emerged as a meaningful clinical signal. Rather than indicating treatment intolerance, peripheral neuropathy appeared to correlate with favorable disease biology and more prolonged treatment exposure. Patients who developed peripheral neuropathy experienced significantly better overall survival (OS) and progression-free survival (PFS) compared with those who did not. Specifically, peripheral neuropathy was associated with a markedly reduced risk of death (HR: 0.16; 95% CI: 0.05–0.56) and disease progression (HR: 0.22; 95% CI: 0.09–0.57).
This pattern suggests that peripheral neuropathy may function as a “tax of efficacy”—patients benefiting from EV+P therapy accumulate more exposure and, consequently, are more likely to develop neuropathy.
The investigators also examined treatment breaks, which were common in this cohort—20 patients required at least one dose interruption. Importantly, treatment breaks did not compromise survival outcomes. Patients who had a treatment break demonstrated a lower risk of death (HR: 0.30; 95% CI: 0.10–0.94) and improved PFS (HR: 0.33; 95% CI: 0.14–0.79) compared with those who continued therapy uninterrupted.
Furthermore, patients who achieved an objective response were substantially more likely to require a treatment break (71% vs 36%) and tended to require breaks earlier during therapy compared with non-responders. This reinforces the interpretation that both peripheral neuropathy and treatment breaks may reflect greater cumulative therapeutic exposure in responding patients, rather than toxicity harming outcomes.
Dr. Yildirim concluded as follows:
- Treatment-emergent peripheral neuropathy functioned as a marker of efficacy rather than a detriment
- Patients who developed peripheral neuropathy demonstrated significantly improved OS and PFS, compared to those who did not.
- Dose interruptions did not negatively impact outcomes, allowing for symptom management without sacrificing efficacy.
- The association between breaks and survival outcomes supports that holding therapy to manage toxicity does not compromise treatment benefit.
Presented by: Ahmet Yildirim, MD, Med, Resident Physician, Department of Internal Medicine, Inova Fairfax Hospital, Falls Church, VA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
Reference: