(UroToday.com) The 2025 SUO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Dingwei Ye discussing intravesical T3011, an IL-12/anti-PD-1 armed oncolytic HSV-1, in BCG-unresponsive high-risk non-muscle invasive bladder cancer. Radical cystectomy remains the standard treatment for high-risk non-muscle invasive bladder cancer patients who experience recurrence after BCG therapy, particularly those classified as BCG unresponsive.
Although effective, radical cystectomy is associated with significant morbidity, underscoring the urgent need for effective bladder-preserving alternatives. Herpes Virus T3011 Injection (MVR-T3011) is a clinical-stage oncolytic HSV-1 designed for cancer immunotherapy. Genetically engineered for tumor-selective replication, it delivers localized expression of two potent immunomodulators: IL-12 and an anti–PD-1 antibody:
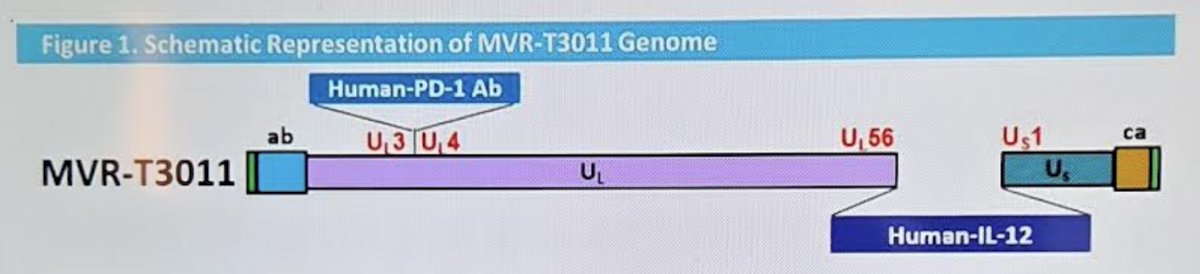
This dual mechanism combines direct oncolysis through viral replication with in situ immune activation, enhancing both local and systemic antitumor immune responses. This study, presented at SUO 2025, aims to evaluate the efficacy and safety of intravesical MVR-T3011 instillation in high-risk non-muscle invasive bladder cancer patients with BCG failure.
BCG unresponsive non-muscle invasive bladder cancer patients were enrolled and treated with intravesical MVR-T3011 at two dose levels: 2 × 109 PFU and 1 × 1010 PFU in a 50 mL solution. To streamline administration, no bladder prewash was performed. At 2 × 109 PFU dose level, MVR-T3011 is administered weekly for 12 weeks as an induction course, and once every 2 weeks for 1 year, then once every 3 weeks until 2 years as a maintenance course. At 1 × 1010 PFU dose level, MVR-T3011 is administered weekly for 6 weeks as an induction course (with a second induction allowed, if applicable) and every 3 weeks until 2 years as a maintenance course. The study design is as follows:
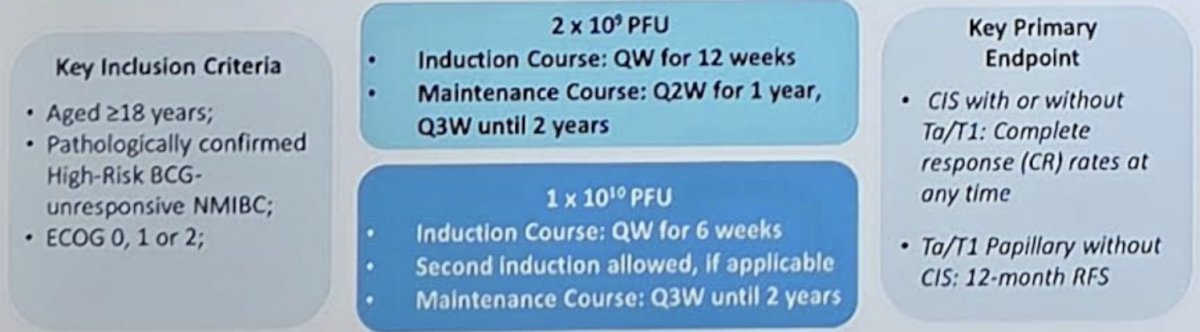
Patients will be evaluated for recurrence and progression using cystoscopy, cytology, biopsy (if applicable), and CT/MRI (if applicable). The primary efficacy endpoints were the complete response rate in patients with CIS and 12-month recurrence-free survival in Ta/T1 without CIS patients.
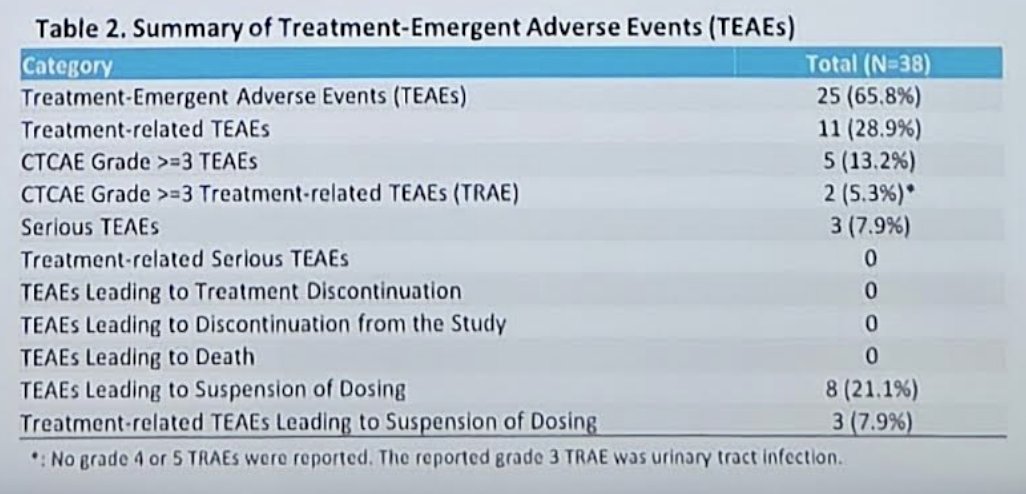
As of the data cutoff, 23 efficacy-evaluable patients received MVR-T3011 at 2 × 109 PFU and 15 received MVR-T3011 at 1 × 109 PFU. There were 25 (65.8%) treatment-emergent adverse events, of which 13.2% were grade 3+ events. Most treatment-emergent adverse events were grade 1, including hematuria (23.4%), urinary tract infection (8.5%), rash (8.5%), proteinuria (8.5%), pollakiuria (4.3%), micturition urgency (2.1%), vomiting (2.1%), and dry mouth (2.1%). Of note, there were no grade 4 or 5 treatment-related adverse events or treatment-related serious adverse events reported:
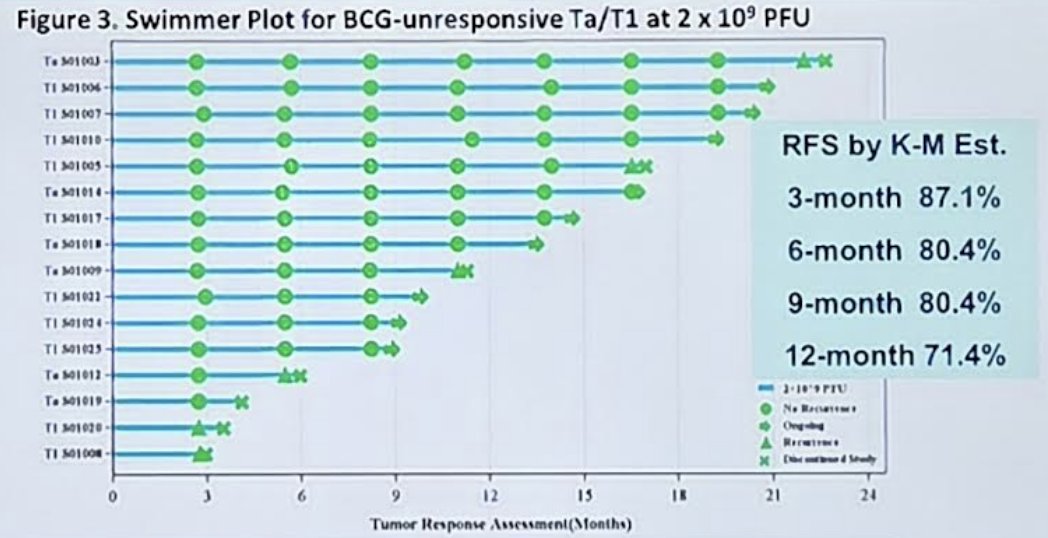
Among patients with BCG-unresponsive Ta/T1 disease, at the MVR-T3011 dose of 2 × 109 PFU, the recurrence-free survival by Kaplan-Meier estimate at 3 months was 87.1%, at 6 months was 80.4%, at 9 months was 80.4%, and at 12 months was 71.4%:
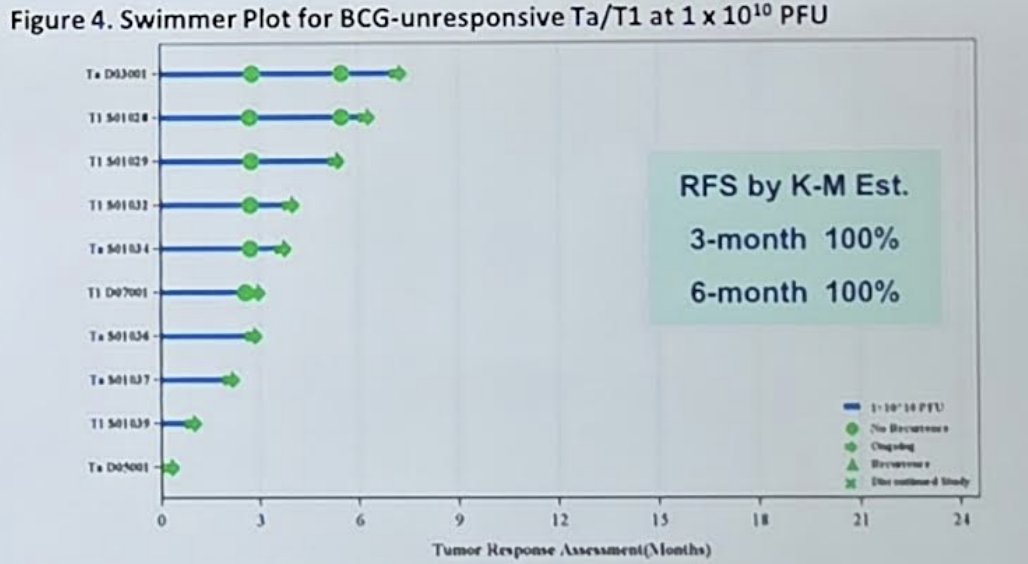
At the MVR-T3011 dose of 1 × 1010 PFU, the recurrence-free survival by Kaplan-Meier estimate at 3 and 6 months was 100%:
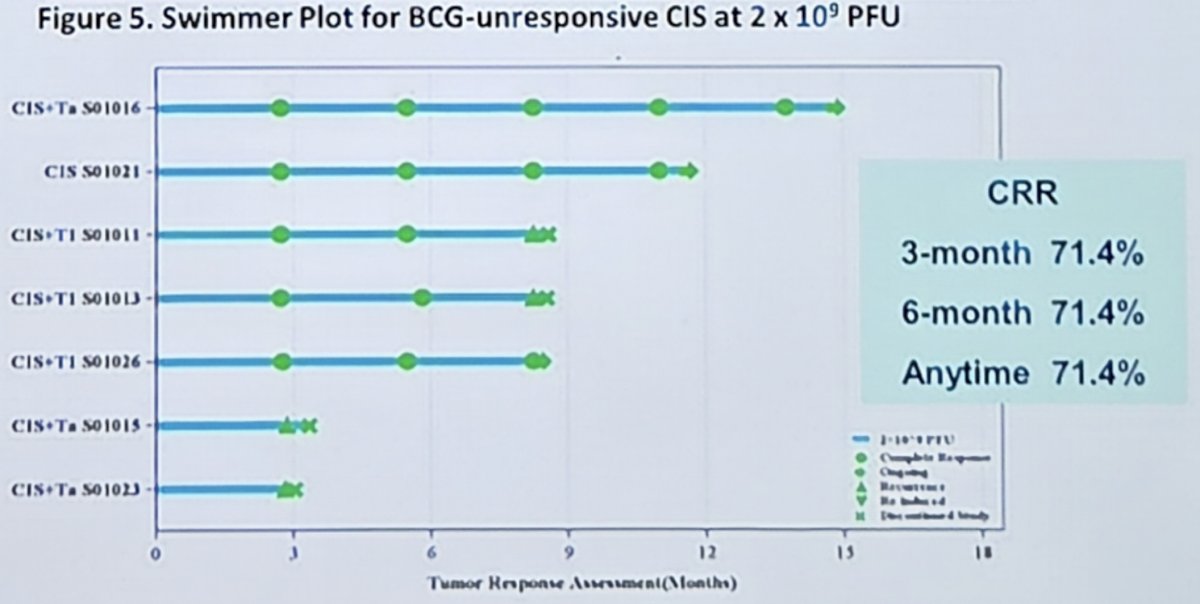
Among patients with BCG-unresponsive CIS, at the MVR-T3011 dose of 2 × 109 PFU, the complete response rate at 3, 6, and anytime was 71.4%:
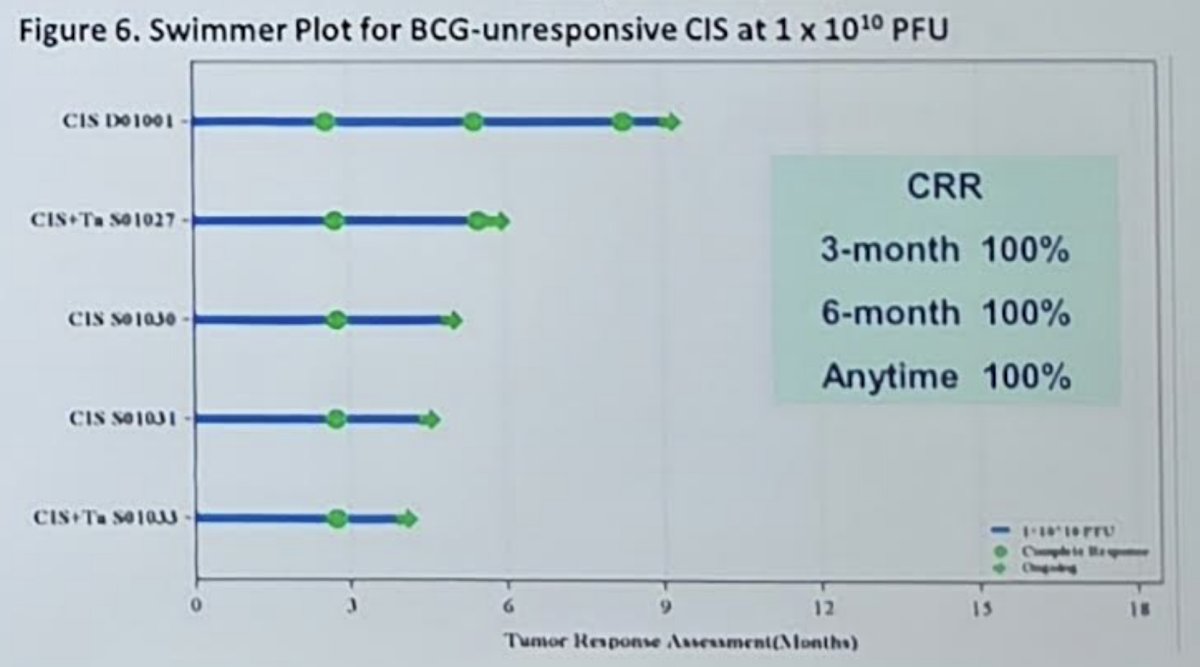
Among patients with BCG-unresponsive CIS, at the MVR-T3011 dose of 1 × 1010 PFU, the complete response rate at 3, 6, and anytime was 100%:
Dr. Ye concluded his presentation discussing intravesical MVR-T3011 in BCG-unresponsive high-risk non-muscle invasive bladder cancer with the following take-home points:
- MVR-T3011 has demonstrated strong potential in the treatment of both CIS and papillary BCG-unresponsive non-muscle invasive bladder cancer
- The administration of MVR-T3011 eliminates bladder prewashing, thereby facilitating clinical application and substantially enhancing patient adherence
Presented by: Dingwei Ye, Fudan University Prostate Cancer Institute, Shanghai, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.