(UroToday.com) The 2025 Society of Urologic Oncology (SUO) annual meeting, held in Phoenix between December 2 and December 5, 2025, was host to the State of the Art Session II: Incorporating Minimal Residual Disease in ctDNA Testing/Assays in Clinical Practice in Bladder Cancer: Are We There Yet? Dr. Gillian Vandekerkhove discussed Technical Advances, Challenges, and Future Directions in Liquid Biopsy MRD Assays.
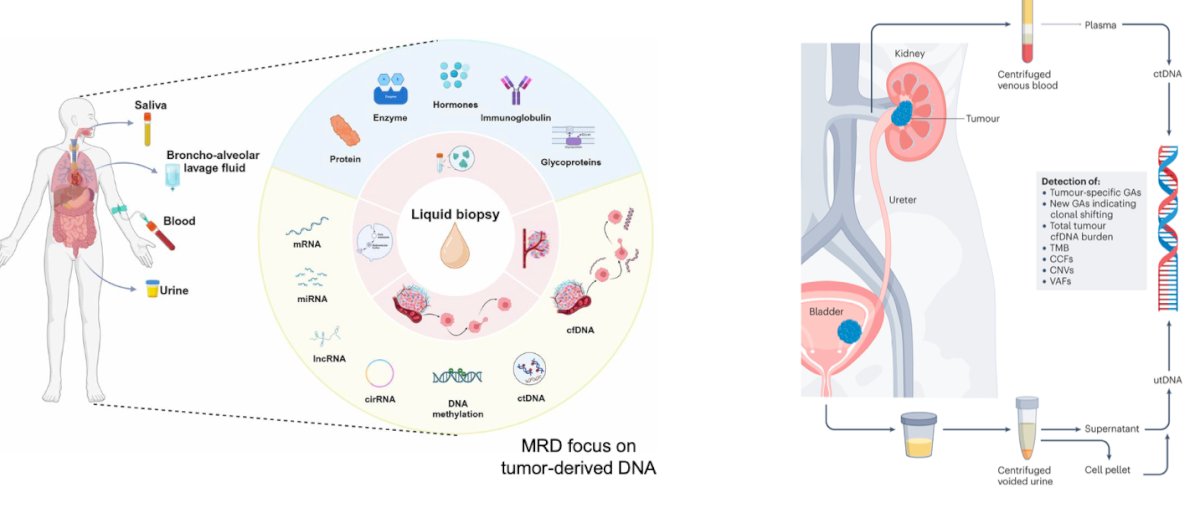
Dr. Vandekerkhove began her presentation by outlining the expanding landscape of liquid biopsy technologies and their relevance across urologic malignancies. She emphasized that liquid biopsies can be derived from multiple biofluids, including blood, urine, saliva, and bronchoalveolar lavage, and enable the capture of a wide spectrum of biomarkers such as proteins, enzymes, immunoglobulins, glycoproteins, mRNA, miRNA, lncRNA, circRNA, cfDNA, and, most importantly, tumor-derived circulating tumor DNA (ctDNA).
He highlighted that ctDNA analysis has gained particular traction for minimal residual disease (MRD) detection, clonal evolution monitoring, and genomic profiling. In urothelial cancer specifically, both plasma-derived ctDNA and urine-derived tumor DNA (utDNA) provide complementary insights into tumor biology, allowing assessment of tumor-specific genomic alterations, mutational burden, copy-number changes, and variant allele fraction dynamics.1
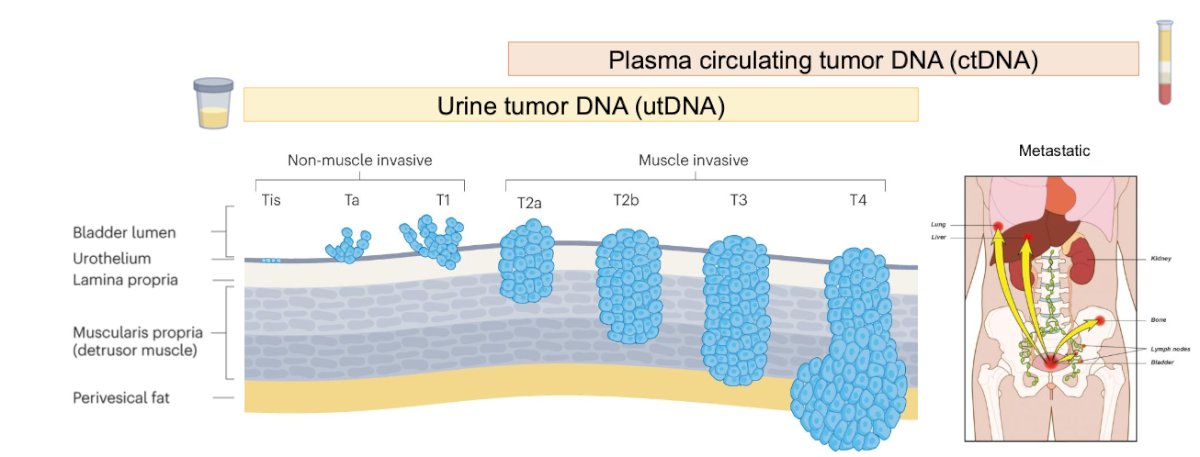
Dr. Vandekerkhove next discussed liquid biopsy biomarkers specifically in urothelial cancer MRD assessment. He emphasized that plasma-derived ctDNA is now a validated blood-based marker of MRD across urothelial and multiple other solid tumors, offering high sensitivity for detecting residual or recurrent disease, particularly in muscle-invasive and metastatic settings. She highlighted that utDNA is emerging as a complementary and potentially more sensitive MRD biomarker for localized urothelial cancer, given its direct contact with the urothelial tract. utDNA may capture tumor-derived alterations across the NMIBC-to-MIBC spectrum and could offer earlier, non-invasive detection of recurrence or progression compared to conventional cystoscopy-based surveillance.2
Moreover, MRD detection relies on highly sensitive assays capable of identifying tumor fractions below 0.01%, far beyond the limits of conventional imaging. MRD assays prioritize detection, not broad genomic profiling using ultra-deep targeted sequencing with sophisticated error-suppression methods, including duplex sequencing. Dr. Vandekerkhove also cautioned that biological background noise, such as clonal hematopoiesis and field cancerization, can introduce non-tumor somatic variants, highlighting the importance of stringent assay design to minimize false-positive results.
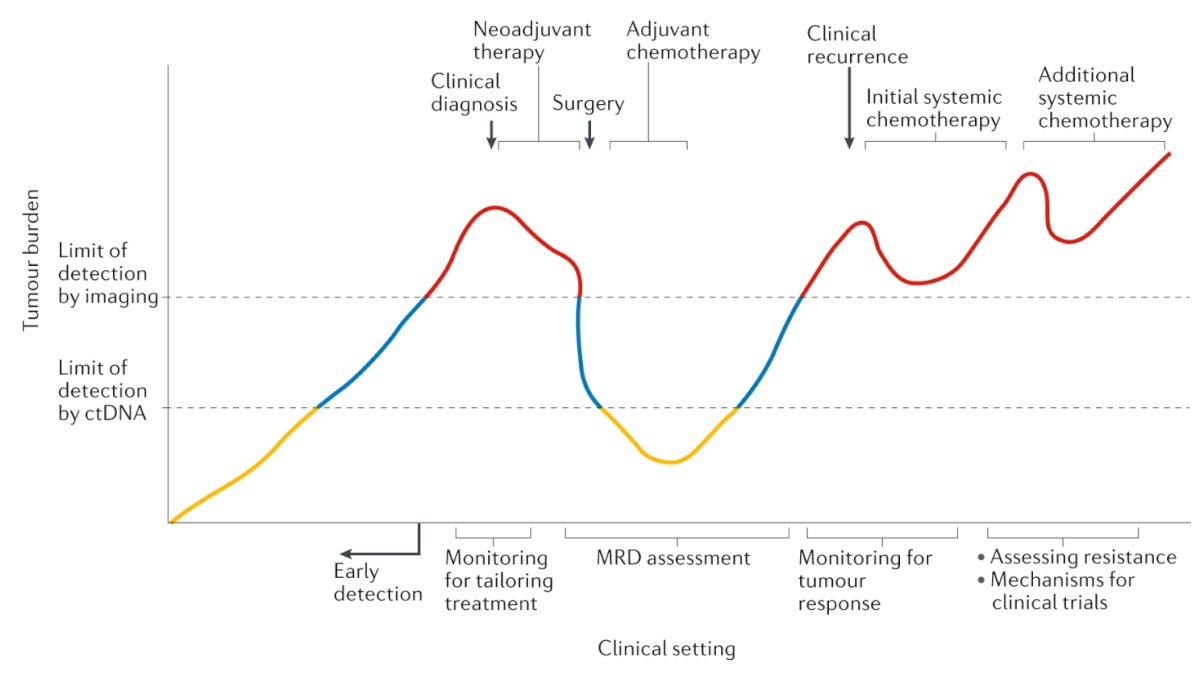
Minimal residual disease serves as a highly sensitive biomarker across multiple phases of the urothelial cancer continuum. Because ctDNA can detect tumor burden well below the limits of imaging, MRD enables earlier detection of microscopic disease, supports treatment tailoring during neoadjuvant and adjuvant therapy, and provides an objective tool for monitoring response after surgery, as illustrated in the figure below.
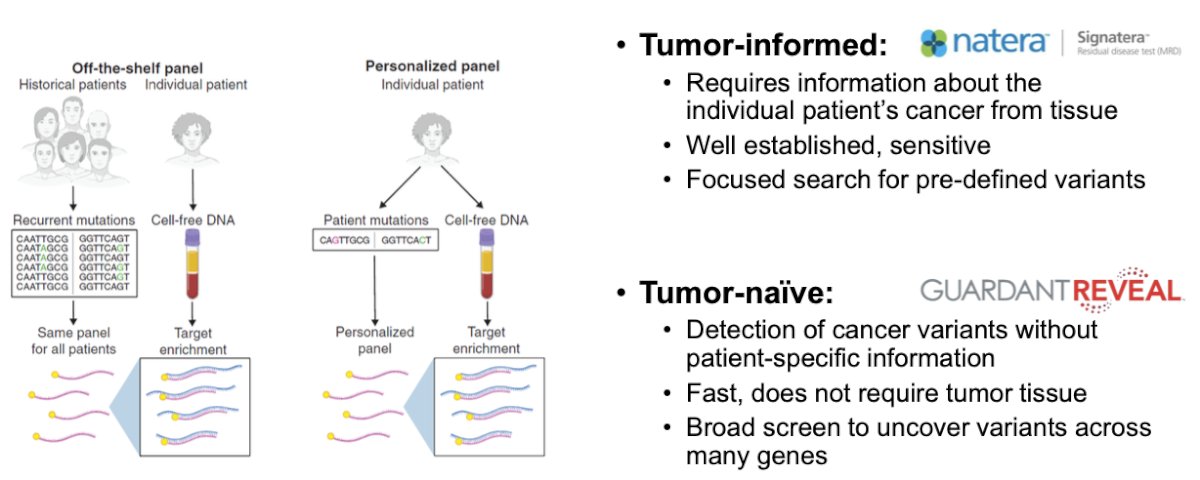
Dr. Vandekerkhove next outlined key distinctions between tumor-informed and tumor-naïve MRD assays. Tumor-informed platforms (such as Signatera) require sequencing of the patient’s tumor tissue to build a personalized mutation panel, enabling highly sensitive and specific detection of predefined variants. In contrast, tumor-naïve assays (such as Guardant Reveal) do not require tumor tissue and instead screen broadly for oncogenic variants directly from plasma, offering faster turnaround and easier implementation, though generally with lower sensitivity for very low-level disease as illustrated below.
Improving MRD assay sensitivity hinges on increasing the likelihood of capturing rare tumor DNA fragments. Strategies include expanding sequencing breadth from WES to whole-genome approaches and increasing depth, integrating additional tumor features such as methylation signals, and boosting input material by collecting larger volumes of blood or urine. She also noted the value of serial testing, which enhances detection through ctDNA kinetic trends over time. These refinements collectively push the limit of detection lower, allowing assays to identify tumor-derived variants well below standard background error rates.3
Dr. Vandekerkhove highlighted how mutation-focused MRD assays continue to evolve, leveraging highly specific detection of SNVs and InDels but facing growing computational demands as sequencing breadth expands. She noted that AI and machine-learning tools are increasingly being incorporated to enhance assay performance, prioritizing whole-genome tissue variants for patient-specific tracking, modeling background noise to push sensitivity below traditional detection thresholds, and integrating DNA mutation data with additional modalities to support a more comprehensive and precise MRD assessment.
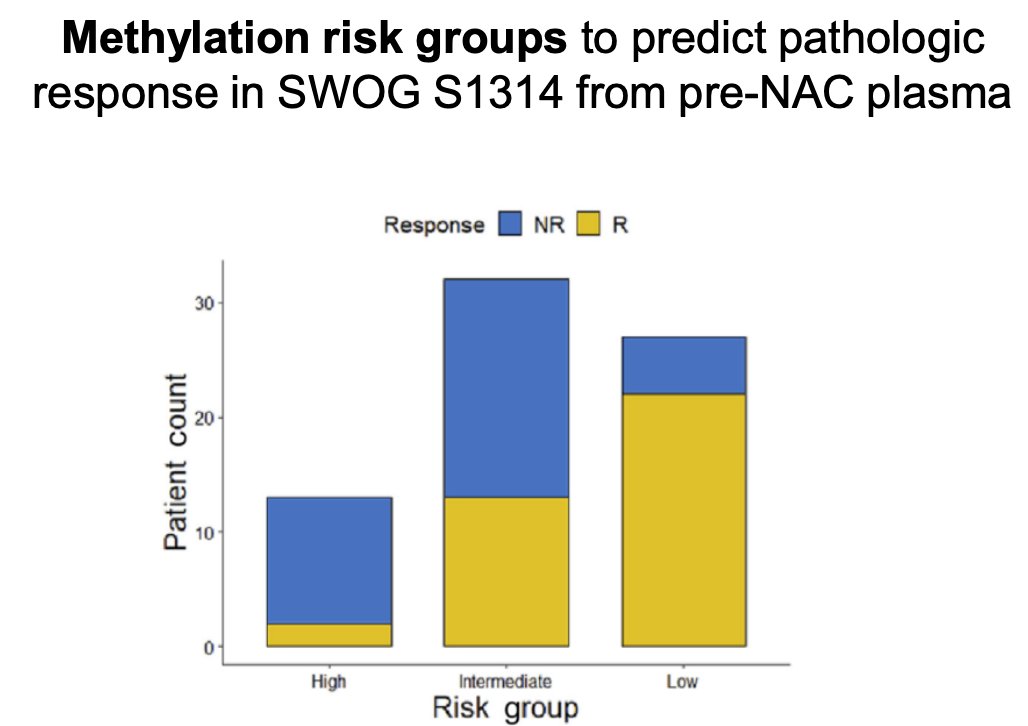
DNA methylation adds a powerful layer of tumor biology to MRD detection, offering richer tumor-derived signals than mutation-only assays. Methylation profiling has the potential to outperform mutation-based MRD tests, and several commercial urine assays already leverage this biology for diagnosis and recurrence monitoring. Because methylation patterns reflect tissue of origin and disease aggressiveness, they can stratify risk and predict treatment response, as demonstrated by methylation risk groups in SWOG S1314 (as shown below). Advances in cfDNA methylation technologies such as cfMeDIP, EM-Seq, and integrated genetic/epigenetic sequencing now enable sensitive profiling from minimal input material, positioning methylation as a key enhancer of MRD detection in urothelial cancer.4
Dr. Vandekerkhove explained that cfDNA fragmentation patterns provide another rich layer of biological information that can enhance MRD detection. Fragmentomics features (as illustrated in the figure below) derived from conventional sequencing data, such as fragment length distributions, nucleosome positioning, and fragment-end signatures, reflect underlying chromatin structure and transcriptional activity. Incorporating these fragment-based signals into MRD assays has been shown to improve sensitivity, offering an orthogonal approach that complements mutation and methylation profiling.

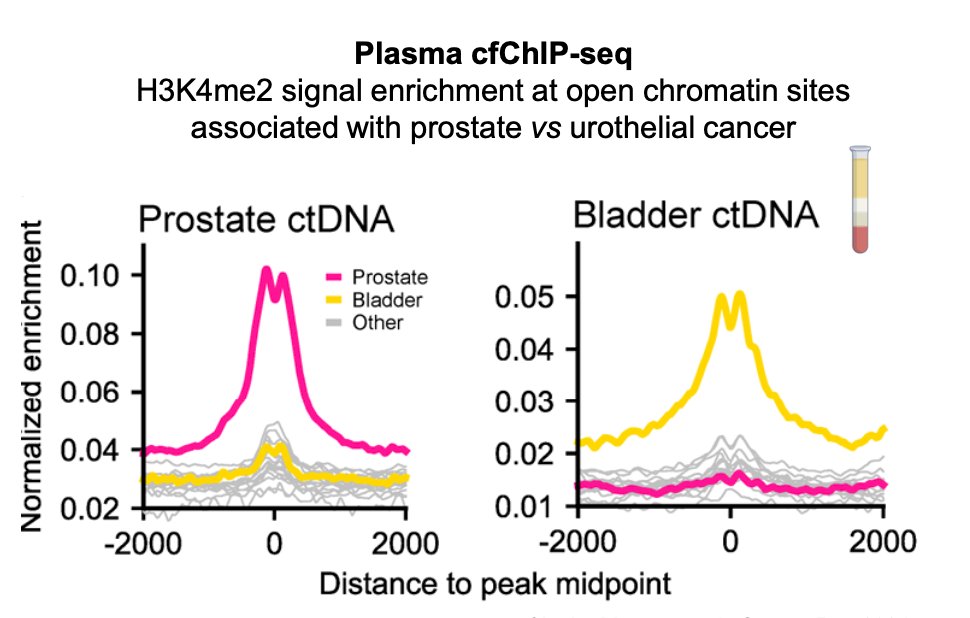
Moreover, cell-free chromatin immunoprecipitation sequencing (cfChIP-seq) allows interrogation of histone modifications preserved in urine and plasma cfDNA, providing insights into the tissue of origin. These histone marks, such as H3K4me1/2/3 and H3K27ac offer complementary biological features that can strengthen multi-omic MRD assays beyond mutation and fragmentation signals. Early studies demonstrate distinct cfChIP-seq enrichment patterns for prostate versus urothelial cancer, supporting its potential to improve tumor classification, enhance MRD sensitivity, and refine disease monitoring in urothelial cancer.5
Liquid biopsy technology has progressed from simple mutation-based assays to increasingly comprehensive platforms that capture multiple dimensions of tumor biology. Early methods focused solely on detecting tumor-derived DNA mutations, but advances in sequencing have enabled broader genomic profiling and the incorporation of epigenomic features such as DNA methylation, fragment length patterns, end motifs, and nucleosome positioning, each contributing additional sensitivity for MRD detection. The field is now shifting toward multi-parameter, multi-omic assays that integrate genomics, fragmentomics, nucleosomics, and methylomics, supported by serial sampling, to provide a more complete and biologically informed assessment of minimal residual disease.
The development of robust MRD assays faces several technical and biological barriers. Because tumor burden is extremely low in the MRD setting, assays must achieve ultra-high sensitivity to reliably detect rare tumor-derived molecules while simultaneously distinguishing true tumor signal from background noise. This is complicated by non-tumor sources of variation, including clonal hematopoiesis in plasma and field cancerization effects in urine. Additional challenges include establishing and validating MRD thresholds for newer epigenomic and multi-omic assays, as well as managing pre-analytic factors that strongly influence assay performance. Current efforts include standardized recommendations for plasma handling and the recently proposed MUMIE framework to guide pre-analytical best practices in urine-based MRD testing.
Lastly, Dr. Vandekerkhove highlighted several key challenges in the interpretation and real-world implementation of MRD testing. Access to MRD technologies remains uneven across regions and health systems, and meaningful adoption requires substantial infrastructure, including sequencing capacity, bioinformatics support, and seamless clinical integration. As technologies rapidly evolve and assays expand to incorporate multi-omic features and longitudinal sampling, the cost and complexity of testing continue to rise. Performance and reporting vary considerably across available platforms, adding further uncertainty. Clinicians must also balance the promise of personalized decision-making with the potential risk of overtreatment driven by increasingly sensitive assays. Importantly, prospective validation remains limited, underscoring the need for robust evidence to guide clinical use.
Dr. Vandekerkhove concluded her presentation with the following key takeaways:
- Urine and plasma enable MRD evaluation in urothelial cancer
- MRD assays are transitioning from limited mutation detection to comprehensive tumor profiling
- Technical improvements and epigenomic technologies promise greater sensitivity
- Artificial intelligence is transforming signal extraction, classification, and multi-omic integration
- Demonstrating clinical utility through prospective studies is essential for implementation
Presented by: Gillian Vandekerkhove, PhD, MSc, Vancouver Prostate Centre, Department of Urologic Sciences, University of British Columbia. Vancouver, BC, Canada.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Penn State Health, @chavarriagaj on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References:- Rose KM, Huelster HL, Meeks JJ, Faltas BM, Sonpavde GP, Lerner SP, Ross JS, Spiess PE, Grass GD, Jain RK, Kamat AM, Vosoughi A, Wang L, Wang X, Li R. Circulating and urinary tumour DNA in urothelial carcinoma - upper tract, lower tract and metastatic disease. Nat Rev Urol. 2023 Jul;20(7):406-419. doi: 10.1038/s41585-023-00725-2. Epub 2023 Mar 28. Erratum in: Nat Rev Urol. 2023 Jul;20(7):452. doi: 10.1038/s41585-023-00783-6. PMID: 36977797.
- Dyrskjøt L, Hansel DE, Efstathiou JA, Knowles MA, Galsky MD, Teoh J, Theodorescu D. Bladder cancer. Nat Rev Dis Primers. 2023 Oct 26;9(1):58. doi: 10.1038/s41572-023-00468-9. PMID: 37884563; PMCID: PMC11218610.
- Moding EJ, Nabet BY, Alizadeh AA, Diehn M. Detecting Liquid Remnants of Solid Tumors: Circulating Tumor DNA Minimal Residual Disease. Cancer Discov. 2021 Dec 1;11(12):2968-2986. doi: 10.1158/2159-8290.CD-21-0634. PMID: 34785539; PMCID: PMC8976700.
- Lu YT, Plets M, Morrison G, Cunha AT, Cen SY, Rhie SK, Siegmund KD, Daneshmand S, Quinn DI, Meeks JJ, Lerner SP, Petrylak DP, McConkey D, Flaig TW, Thompson IM Jr, Goldkorn A. Cell-free DNA Methylation as a Predictive Biomarker of Response to Neoadjuvant Chemotherapy for Patients with Muscle-invasive Bladder Cancer in SWOG S1314. Eur Urol Oncol. 2023 Oct;6(5):516-524. doi: 10.1016/j.euo.2023.03.008. Epub 2023 Apr 20. PMID: 37087309; PMCID: PMC10587361.
- Sipola J, Munzur AD, Kwan EM, Seo CCY, Hauk BJ, Parekh K, Liao YJR, Bernales CQ, Donnellan G, Bloise I, Fung E, Ng SWS, Wang G, Vandekerkhove G, Nykter M, Annala M, Maurice-Dror C, Chi KN, Herberts C, Wyatt AW, Takeda DY. Plasma Cell-Free DNA Chromatin Immunoprecipitation Profiling Depicts Phenotypic and Clinical Heterogeneity in Advanced Prostate Cancer. Cancer Res. 2025 Feb 17;85(4):791-807. doi: 10.1158/0008-5472.CAN-24-2052. PMID: 39652574; PMCID: PMC11832346.