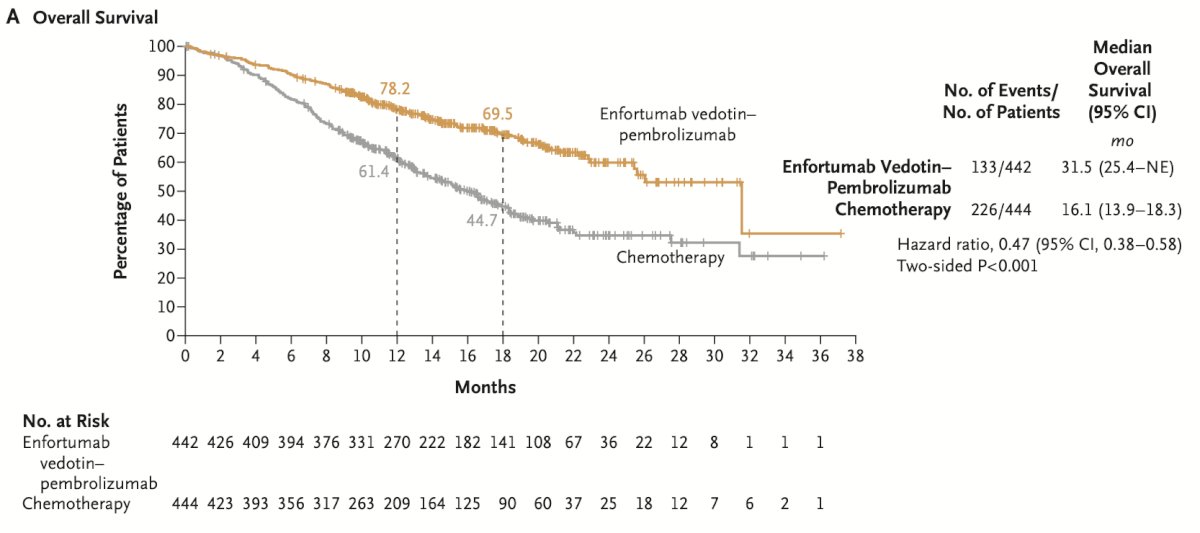
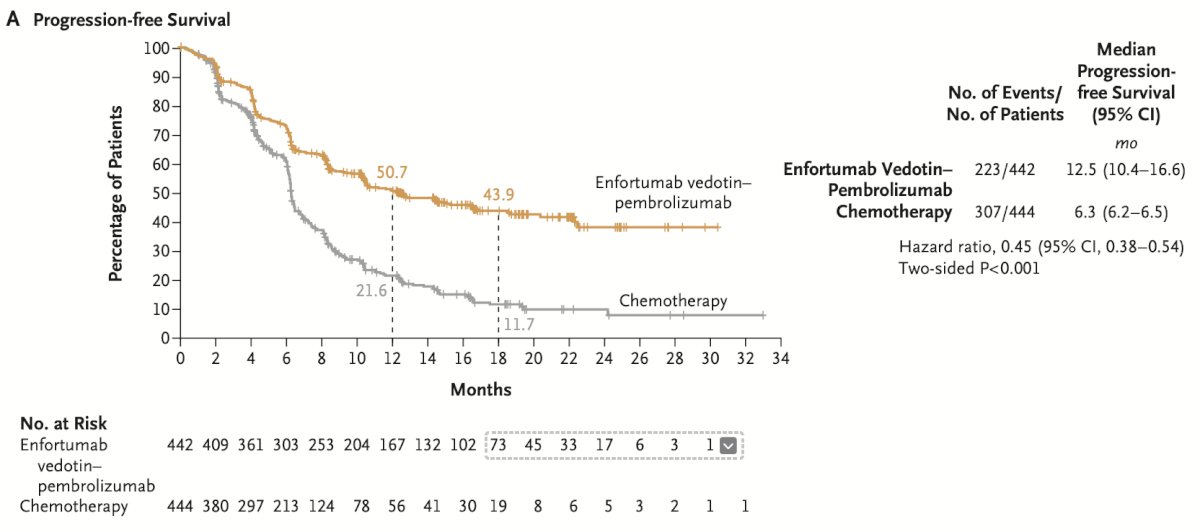
(UroToday.com) The 2025 SUO annual meeting featured a urothelial carcinoma trials in progress session and a presentation by Dr. Abdul Qadar discussing CT-READ, a study assessing circulating tumor DNA (ctDNA) response adapted treatment de-escalation in metastatic urothelial carcinoma. Metastatic urothelial carcinoma remains a lethal malignancy with a 5-year survival rate below 10%, despite recent therapeutic advances. Recent landmark trials EV-103 and EV-302 have led to a paradigm shift, demonstrating significant improvements in overall survival and progression free survival with pembrolizumab + enfortumab vedotin combination as front-line therapy.1 These trials have established pembrolizumab + enfortumab vedotin as a new standard of care, with the EV-302 study reporting a median overall survival of 31.5 months and a median progression free survival of 12.5 months:
Despite these outcomes, the front-line pembrolizumab + enfortumab vedotin regimen is associated with high rates of treatment related adverse events. In EV-302, 56% of patients experienced ≥ grade 3 treatment related adverse events, leading to dose reductions in 40.7% and discontinuation in 35%. Importantly, clinical benefit persisted after therapy cessation, highlighting the need for predictive biomarkers to guide safe de-escalation. Immune checkpoint inhibitors are well tolerated but have limited and short-lived efficacy as monotherapy without favorable molecular predictors. Common biomarkers such as PD-L1 expression often produce inconsistent results and are hindered by intra-tumor and temporal variability.
ctDNA has emerged as a dynamic, minimally invasive biomarker that reflects tumor burden and treatment response across malignancies. In metastatic urothelial carcinoma, prospective studies have shown ctDNA to be a strong predictor of radiographic response and survival outcomes. Reductions in ctDNA levels of ≥50% have been independently associated with improved progression free survival and overall survival, regardless of PD-L1 or tumor mutational burden status.
Dr. Qadar and colleagues recently analyzed prospectively collected ctDNA for 10 metastatic urothelial carcinoma patients at their institution receiving front-line pembrolizumab + enfortumab vedotin. They found that 70% of patients achieved ≥50% ctDNA reduction, and 40% achieved ctDNA clearance. All patients without a decrease in ctDNA experienced disease progression, while all patients with a ≥50% reduction sustained responses for 4–12 months. Notably, five patients who underwent enfortumab vedotin de-escalation due to treatment related adverse events but had a ≥50% ctDNA reduction maintained durable responses on pembrolizumab monotherapy.
These data provide a compelling rationale for a de-escalation strategy guided by ctDNA kinetics. This prospective, investigator-initiated pilot trial aims to test the hypothesis that patients achieving a ≥50% reduction in ctDNA after 6 months of front-line pembrolizumab + enfortumab vedotin can safely de-escalate to pembrolizumab monotherapy without compromising disease control. The findings will provide preliminary efficacy, safety, and biomarker correlation data to inform a larger, biomarker-driven randomized controlled trial.
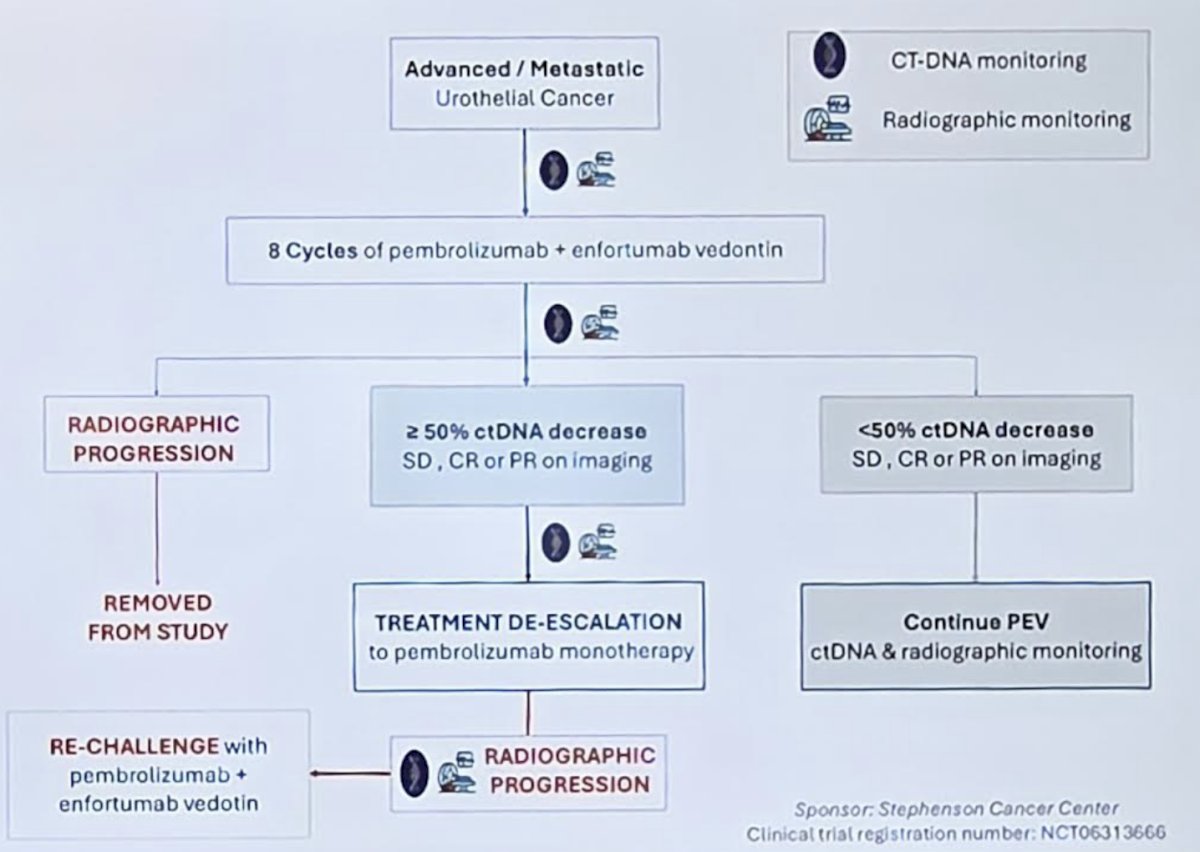
This is a single-institution, single-arm, open-label, phase II pilot trial (NCT06313666) evaluating biomarker-driven treatment de-escalation in patients with metastatic urothelial carcinoma treated with front-line pembrolizumab + enfortumab vedotin. The primary objective is to evaluate progression free survival at 3 and 6 months following de-escalation to pembrolizumab monotherapy in patients who achieve ≥50% reduction in ctDNA after 6 months (8 cycles) of standard front-line pembrolizumab + enfortumab vedotin.
The trial utilizes a Simon two-stage minimax design to assess whether the de-escalation strategy meets the efficacy threshold to warrant further evaluation. The investigators anticipate that by enrolling 30 patients on the trial, 21 patients will be eligible for de-escalation, and after accounting for a 10% attrition, there will be 19 evaluable patients on de-escalated therapy. The pilot trial will be considered successful if 7 or more patients remain progression-free at 3 months following de-escalation. The analysis will encompass the evaluation of tolerability and efficacy endpoints across the entire cohort of patients administered any dosage of front-line pembrolizumab + enfortumab vedotin.
All participants will receive standard of care front-line pembrolizumab + enfortumab vedotin for 8 cycles. Blood will be collected at baseline and every 12 weeks for ctDNA analysis using a tumor informed bespoke multiplex PCR ctDNA assay. Patients demonstrating ≥50% reduction in ctDNA at the 6-month mark without radiographic evidence of progression will discontinue enfortumab vedotin and continue pembrolizumab monotherapy every 6 weeks until progression or unacceptable toxicity. Upon progression, patients will be re-challenged with enfortumab vedotin:
Mandatory baseline tumor tissue samples will undergo whole exome sequencing. Additional correlative endpoints include tracking of resistance mechanisms through ctDNA mutational profiling, assessment of ctDNA clearance, and correlation of ctDNA kinetics with radiographic imaging.
The investigators will also evaluate peripheral neuropathy using a multimodal approach. This includes using the FACT-NTX-12 patient-reported outcome tool, as well as the hallux extension strength testing using QuHalEx, an OU-patented load-cell device capable of detecting motor deficits not captured by traditional manual muscle testing. Data from this trial will inform feasibility, safety, and biomarker validation for ctDNA-guided treatment de-escalation in metastatic urothelial carcinoma and lay the foundation for a future randomized trial.
Key inclusion criteria include histologically confirmed unresectable or metastatic urothelial carcinoma, ECOG ≤2, measurable disease per RECIST 1.1, and receipt of ≤1 prior systemic therapy. Patients must be eligible for pembrolizumab + enfortumab vedotin and have adequate organ function. Exclusion criteria include prior immune checkpoint inhibitor or enfortumab vedotin exposure, active autoimmune disease, or untreated CNS metastases.
Presented by: Abdul Qadar, MD, University of Oklahoma, Oklahoma City, OK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References: