(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a bladder cancer poster session. Dr. Joshua Meeks presented a qualitative study of the SunRISe trial investigators’ experiences with TAR-200 in high-risk (HR), non-muscle invasive bladder cancer (NMIBC).
Gemcitabine intravesical system (Gem-iDRS) is a novel intravesical gemcitabine therapy that has recently been approved by the FDA for BCG-unresponsive NMIBC with carcinoma in situ with or without papillary tumors and is under investigation for additional indications, including BCG-naïve, HR-NMIBC, and BCG-experienced HR-NMIBC. Results from the SunRISe-1 phase 2b trial demonstrate a favorable safety profile and durable complete responses with Gem-iDRS monotherapy,1 addressing a significant unmet need for patients who are ineligible for or who decline radical cystectomy. This study aimed to qualitatively understand the treatment experiences and clinical practices of trial investigators, which could inform future clinical practice and enhance the management of patients treated with Gem-iDRS for NMIBC.
Healthcare providers (HCPs) specializing in urology who participated in the SunRISe-1 or SunRISe-3 trials in the United States and allied healthcare professionals (AHCPs) who assisted these HCPs during SunRISe trials were invited to participate in virtual, 60-minute, semi-structured, open-ended, 1-on-1 qualitative interviews between April and June 2025.
Interviews elicited HCPs’ practices in Gem-iDRS preparation, insertion, removal, monitoring, management of adverse events (AEs), care model designs, and their perceived future practice patterns with Gem-iDRS in a real-world setting. The study sponsor was blinded to the identity of the HCPs and AHCPs included in the research. The interviews were audio-recorded, and transcripts were coded using NVivo qualitative data analysis software. The results were analyzed in aggregate and summarized descriptively.
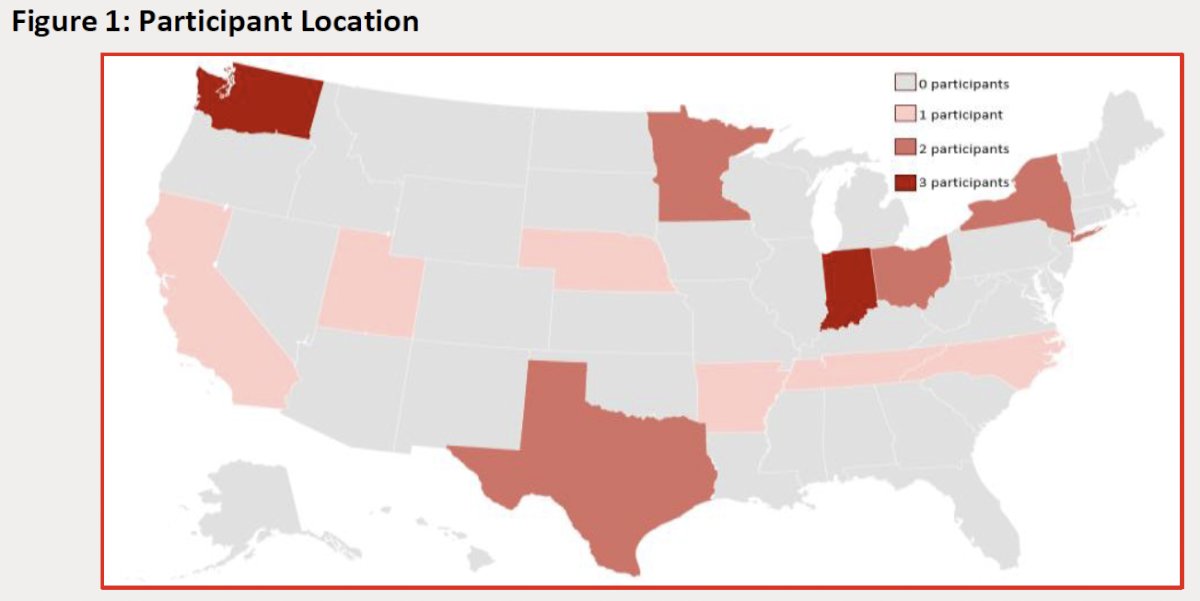
Eighteen unique HCPs from 13 U.S. states and six AHCPs from five practices completed interviews.
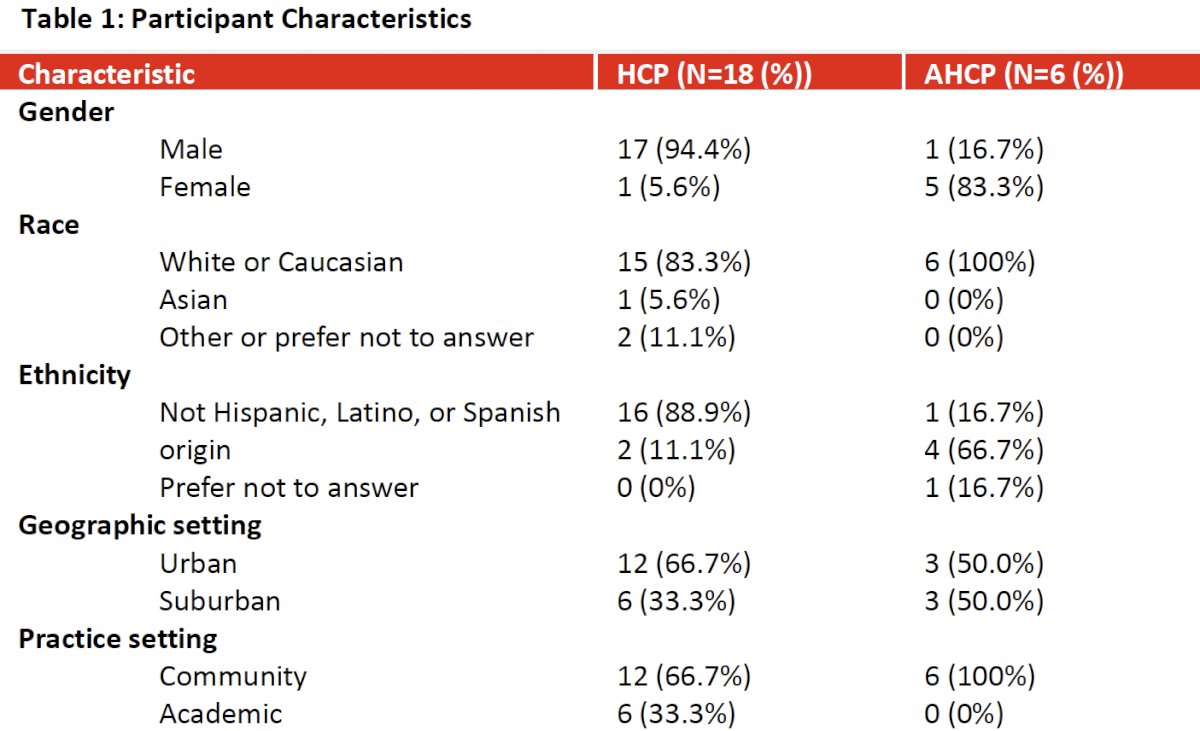
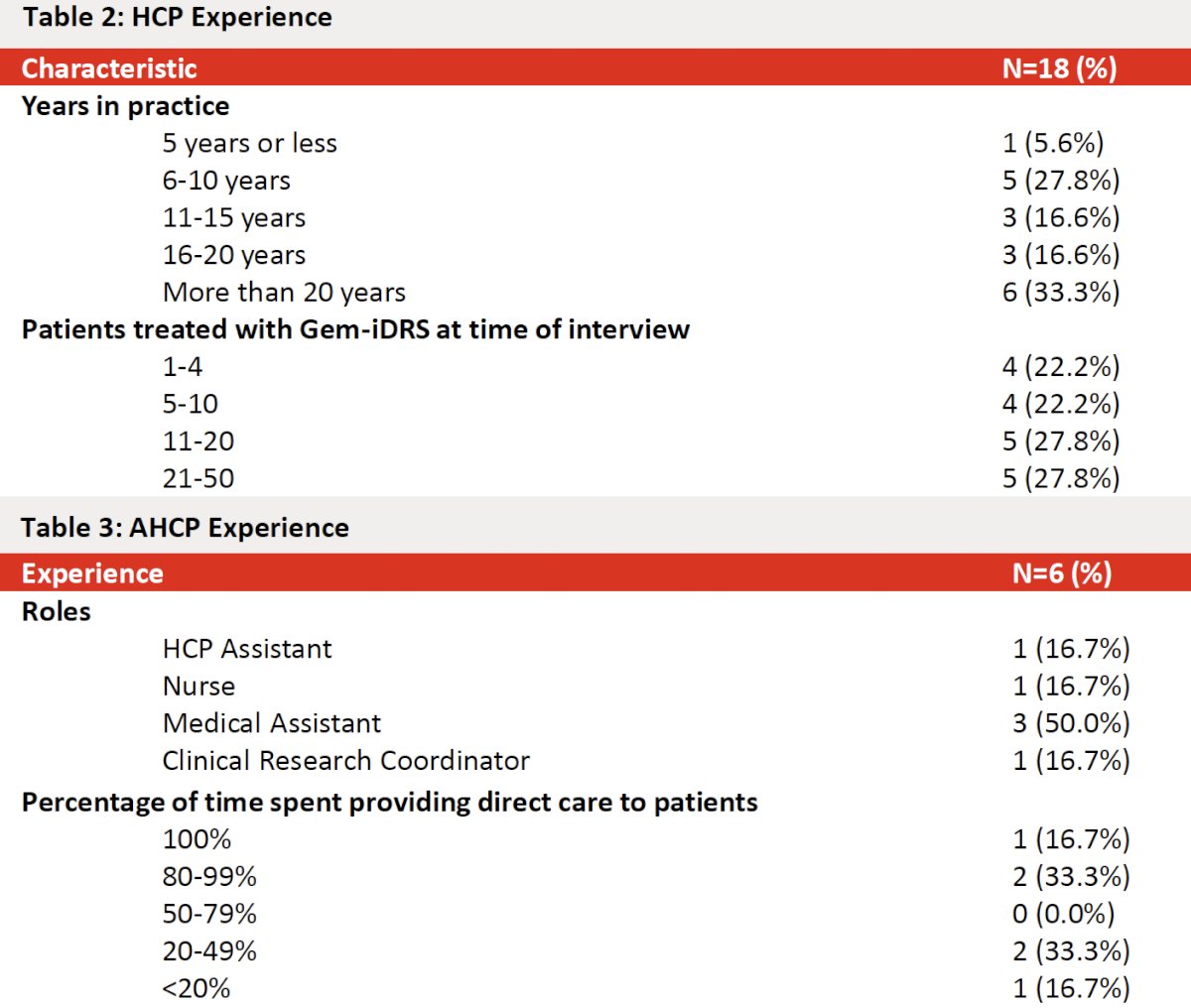
HCP experience varied: 33.3% had >20 years in practice, 27.8% had 6–10 years, and the remainder were distributed across earlier career stages. At the time of interview, HCPs reported treating a range of patients with Gem-iDRS: 22.2% had treated 1–4 patients, 22.2% 5–10, 27.8% 11–20, and 27.8% 21–50 patients. Demographics of interviewed HCPs were predominantly male (94.4%) and White (83.3%); AHCP respondents were more commonly female (83.3%). Most HCPs practiced in community settings (66.7%) and two-thirds were located in urban settings.
Preparation, insertion, removal, and workflow
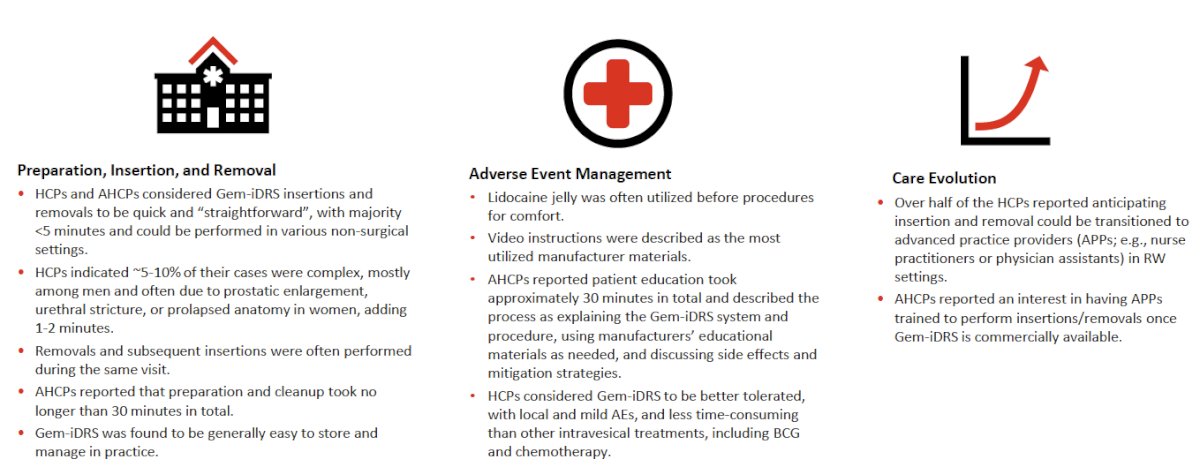
HCPs and AHCPs described insertion and removal as fast, straightforward procedures in most patients, typically taking less than 5 minutes for placement and under 1 minute for removal. Most cases (~95%) were uncomplicated; approximately 5–10% were considered more complex (e.g., large prostate, urethral stricture, or pelvic anatomy issues), with complexity adding 1–2 minutes to the procedure. AHCPs reported that overall preparation and cleanup required ≤30 minutes per visit. Removals and re-insertions were commonly performed during the same visit. Providers emphasized that Gem-iDRS can be performed in a variety of non-operating room settings, increasing its feasibility for many clinics.
Patient Comfort, Education, and Materials
Lidocaine jelly was commonly used pre-procedure for patient comfort. AHCPs estimated that patient education took roughly 30 minutes, using manufacturer materials and video instructions as core resources. Video materials were described as the most utilized educational tool. HCPs perceived the in-clinic education and short procedure time as acceptable to patients and staff.
Tolerability and Adverse Events
Across investigators, Gem-iDRS was characterized as well tolerated with primarily local, low-grade urinary symptoms. HCPs most commonly reported frequency, urgency (pollakiuria), dysuria, and hematuria as expected and manageable AEs. Interviewees noted there were no novel systemic toxicity signals to monitor beyond usual intravesical effects; most AEs were described as mild and amenable to conservative management. The overall perception was that Gem-iDRS is tolerated better and is less time-intensive for patients than conventional intravesical regimens (e.g., weekly instillations), reducing travel frequency and chair time.
Comparisons with Existing Intravesical Options and Perceived Benefits
Investigators repeatedly contrasted Gem-iDRS favorably against conventional intravesical chemotherapy and BCG for several practical reasons: sustained 24/7 intravesical exposure versus short-dwell instillations, fewer clinic visits (e.g., every 3 weeks vs weekly induction), simpler storage/handling, and reduced nursing burden. Several interviewees highlighted potential adoption advantages for patients living at a distance and for smaller practices where frequent visits impose logistical challenges. Many HCPs suggested that advanced practice providers (APPs) could be trained to perform insertions and removals in routine practice, enhancing scalability.
Select HCP participant quotations for key domains are summarized below:
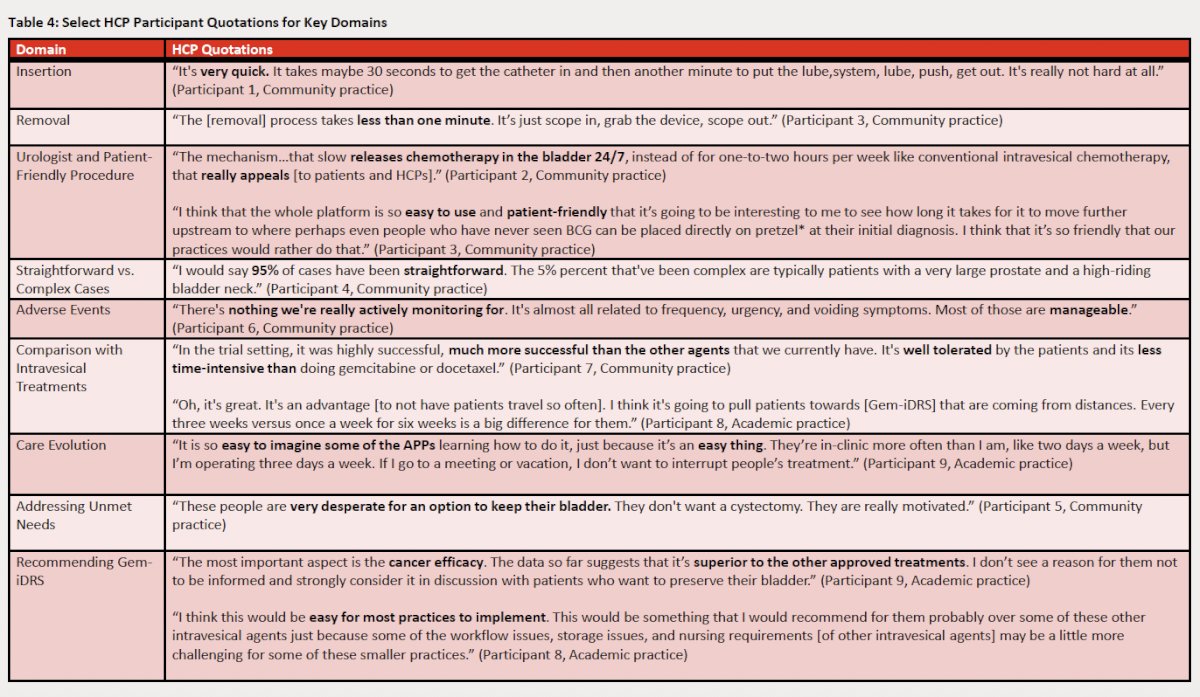
Dr. Meeks did note that this work is qualitative and descriptive with a relatively modest sample size (18 HCPs, 6 AHCPs) and inherent selection bias—participants were SunRISe trial investigators and thus likely early adopters with high familiarity. The findings reflect perceived experiences rather than prospective comparative effectiveness or safety data. Several authors and many participants disclosed relationships with the manufacturer, and the sponsor provided educational materials; the sponsor was blinded to individual participant identities, but industry ties remain a potential source of bias. Finally, patient perspectives were not included in this study and will be critical to fully understand acceptability and quality-of-life impacts.
Dr. Meeks concluded as follows:
- The study findings suggest that the insertions and removals of Gem-iDRS are generally perceived as straightforward, efficient, and feasible across various clinical settings, as reported by the HCPs and AHCPs participating in the trial
- Trial investigators considered Gem-iDRS to be better tolerated, with local and mild adverse events, and less time-consuming than other intravesical treatments, including BCG and chemotherapy.
- These findings complement the previously reported clinical trial data and suggest that Gem-iDRS could offer a treatment approach that is both patient- and provider-friendly.
- Alongside clinical trial data, results from this qualitative study support that Gem-iDRS could address unmet needs in NMIBC by providing a novel therapeutic option that improves the experiences of HCPs and patients.
Presented by: Joshua J. Meeks, MD, PhD, Oncologist, Associate Professor of Urology, Biochemistry and Molecular Genetics, Northwestern University Feinberg School of Medicine, Jesse Brown VA Medical Center in Chicago, Chicago, IL
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
- Daneshmand S, Van der Heijden MS, Jacob JM, et al. TAR-200 for Bacillus Calmette-Guérin–Unresponsive High-Risk Non–Muscle-Invasive Bladder Cancer: Results From the Phase IIb SunRISe-1 Study. J Clin Oncol. 2025; 43(33): 3578-88.