(UroToday.com) The 2025 SUO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Mark Tyson discussing 24 month outcomes from BOND-003 Cohort C, a phase 3 study of intravesical cretostimogene grenadenorepvec for high-risk BCG-unresponsive non muscle invasive bladder cancer with CIS. A significant treatment gap exists for efficacious, well-tolerated bladder sparing options for patients with high-risk BCG unresponsive non muscle invasive bladder cancer with CIS +/- HG Ta/T1. BCG unresponsive disease is defined as persistent or recurrent CIS +/- Ta/T1 within 12 months of BCG therapy, per FDA guidance. Cretostimogene grenadenorepvec is a tumor-selective oncolytic immunotherapy with a dual mechanism of action. It replicates in and lyses cancer cells with Retinoblastoma-E2F pathway alterations, leading to tumor antigen release and anti-tumor immune response, further amplified by the GM-CSF transgene. BOND-003 is a phase-3 study evaluating the efficacy and safety of cretostimogene in patients with high-risk BCG unresponsive non muscle invasive bladder cancer with CIS +/- HG Ta/T1 (Cohort C) and HG Ta/T1 only (Cohort P). At the 2025 SUO annual meeting, Dr. Tyson and colleagues reported updated 24 month outcomes from Cohort C. Notably, cretostimogene has received FDA fast track and breakthrough therapy designations for BCG unresponsive non muscle invasive bladder cancer with CIS.
A total of 112 adults with confirmed high-risk BCG unresponsive non muscle invasive bladder cancer with CIS were enrolled, with efficacy data from 110 patients. All visible disease was resected prior to treatment. Participants had previously received adequate BCG and were considered BCG unresponsive by the US FDA guidance. Cretostimogene treatment consisted of 6 weekly doses during induction, followed by 3 weekly maintenance cycles at months 3, 6, 9, 12, and 18:

Participants were eligible for repeat induction therapy at month 3 if persistent high grade Ta or CIS was noted at biopsy. Response assessment included cystoscopy (biopsy as indicated) and cytology every 3 months for the first 2 years and every 3 months starting year 3, with centralized review of all pathology. The primary endpoint was complete response at any time. Secondary endpoints included duration of response, recurrence free survival, progression free survival, cystectomy free survival, safety, and tolerability.
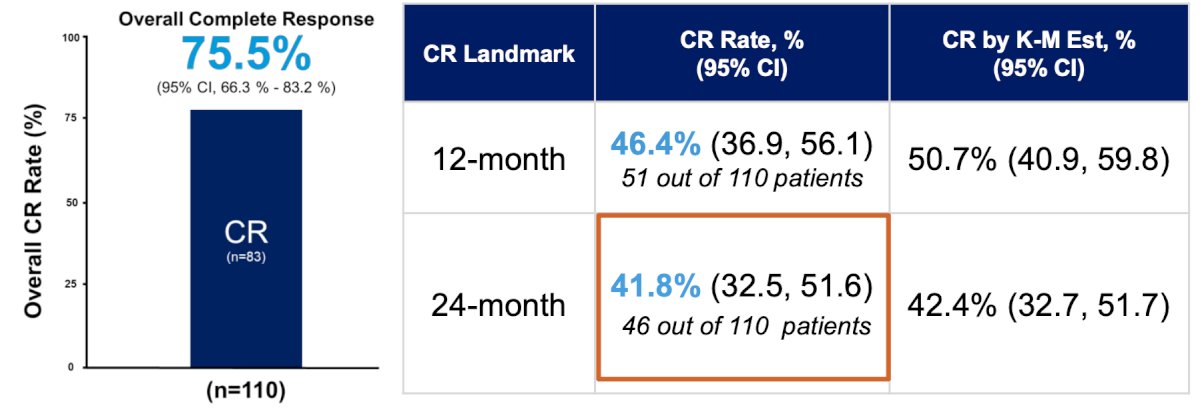
As of the June 23 2025, data cutoff, with a median follow-up time of 25.8 months, the complete response rate at any time is 75.5% (83/110) (95% CI 66.3-83.2%). The 12 month complete response rate is 46.4% (51/110) (95% CI 36.8-56.1%). Updated results include landmark and Kaplan Meier estimated 24 month complete response rates of 41.8% (46/110) (95% CI 32.5-51.6%) and 42.4% (95% CI 32.7–51.7%), respectively. Therefore, 90% of 12-month responders maintained durable outcomes at year 2, and complete responses are consistent across all patient subgroups:
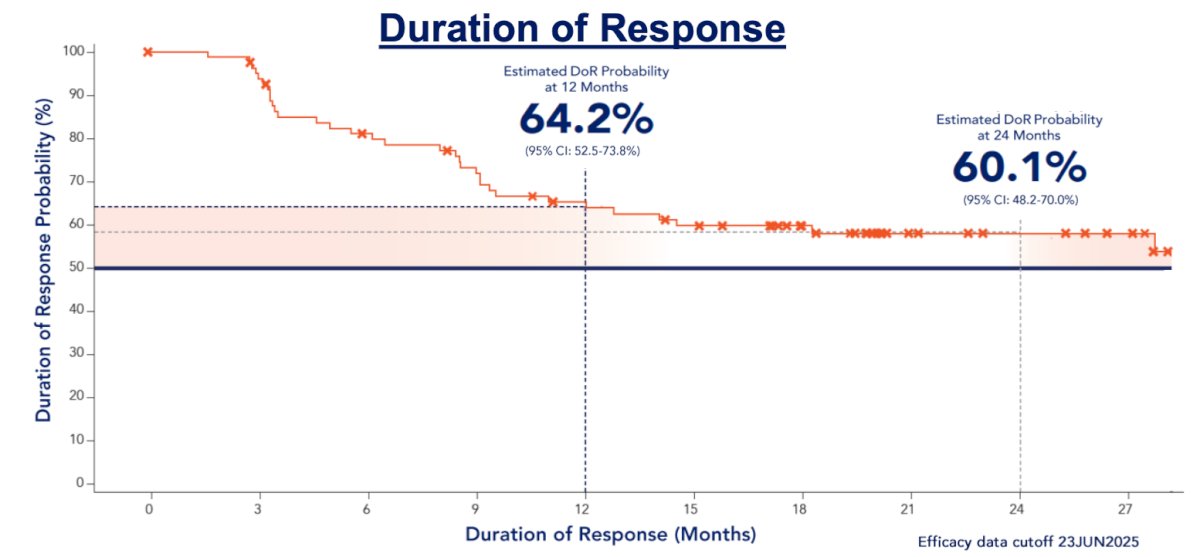
Kaplan-Meier estimates of 12 and 24 month duration of response are 64.2% (95% CI 52.5-73.8%) and 60.1% (95% CI 48.2-70.0%), respectively, with an ongoing median duration of response of 27.9 months (95% CI 14.3-NE%) and is ongoing:
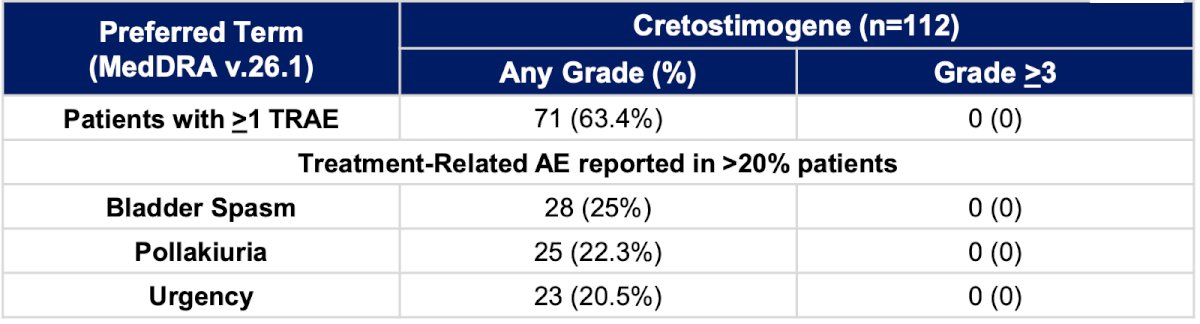
At 24 months, 96.4% (106/110) are free from ≥T2 progression during the treatment phase, and 83.6% (92/110) have avoided a radical cystectomy for bladder cancer. Overall, 83.3% (15/18) of patients who underwent radical cystectomy had T0 or non muscle invasive bladder cancer. Cretostimogene has a very well-tolerated safety profile, with no grade ≥3 treatment-related adverse events. Grade 1 and 2 related adverse events are transient, with a median resolution time of 1 day:
Additionally, there was high treatment compliance with no treatment related discontinuations, and few missed (1.8%) or delayed (7.1%) doses.
Dr. Tyson concluded his presentation discussing 24-month outcomes from BOND-003 Cohort C with the following take home points:
- Cretostimogene offers distinct advantages with its efficacy, durability, and safety profile for the treatment of high-risk BCG-unresponsive non muscle invasive bladder cancer
- Ongoing and future investigations of this promising therapy, as monotherapy and in rational combinations, may address the considerable unmet need for patients with bladder cancer
Presented by: Mark Tyson, MD, MPH, Mayo Clinic, Phoenix, AZ
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
Related Content:
24-Month Follow-Up Data from Phase 3 BOND-003 Cohort C Trial - Mark Tyson