(UroToday.com) At the Annual Meeting of the Society of Urologic Oncology (SUO), there was a session focused on prostate specific membrane antigen (PSMA) and prostate cancer. In the context of this session, Dr. Karen Elizabeth Hoffman presented the evolving role of theranostics in high-risk localized prostate cancer.
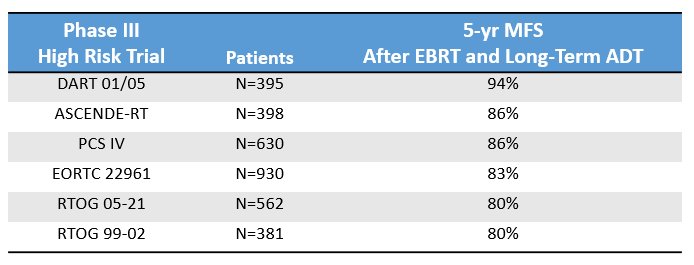
Dr. Hoffman began by emphasizing that standard treatments including radical prostatectomy or radiotherapy with androgen deprivation therapy (ADT) are not sufficient for a subset of patients with localized high risk disease. Accordingly, biochemical recurrence rates range from 20% up to 50% of these patients by five-years after treatment, with varying rates according to oncologic risk. While biochemical recurrence represents an important clinical endpoint, even more importantly, she emphasized that these patients are at substantial risk of metastatic progression. Across a number of trials assessing external beam radiotherapy with ADT, she emphasized that 5-year metastasis free survival is approximately 85%, with some variation according to patient cohorts and treatment paradigms.
It’s clear that a large driver of this metastatic progression is undertreatment of microscopic disease present at the time of initial treatment. Thus, further treatment of microscopic disease, such as in the pelvic lymph nodes, should improve survival. This hypothesis was tested and found to be true, in the POP-RT trial which enrolled patients with clinically-node negative high-risk prostate cancer who, based on pre-treatment nomogram, were estimated to have at least a 20% risk of nodal involvement. The addition of whole pelvic radiotherapy to prostate radiation, was associated with improvements in biochemical failure-free survival, disease-free survival, and metastasis-free survival, with an absolute difference of 7% (96% vs 89%) at 5-years. These improvements relied upon improved delivery of current treatments. However, there is the potential for further benefit from the integration of novel treatment paradigms.
To that end, Dr. Hoffman discussed the potential for theranostic radiation delivery to address micrometastatic disease in patients with high-risk prostate cancer, with obviously open and unanswered questions regarding the integration with current treatment paradigms including radical prostatectomy and radiotherapy.
Considering these approaches, she first highlighted the LuTectomy study. This is a single-arm, feasibility study aimed at assessing the dosimetry, feasibility, and potential benefit of neoadjuvant administration of 177Lu-PSMA-617 prior to radical prostatectomy in patients with biopsy proven prostate cancer with high-risk features but no clinical evidence of distant metastatic disease. Patients must have high PSMA update (SUVmax >20) to be eligible.
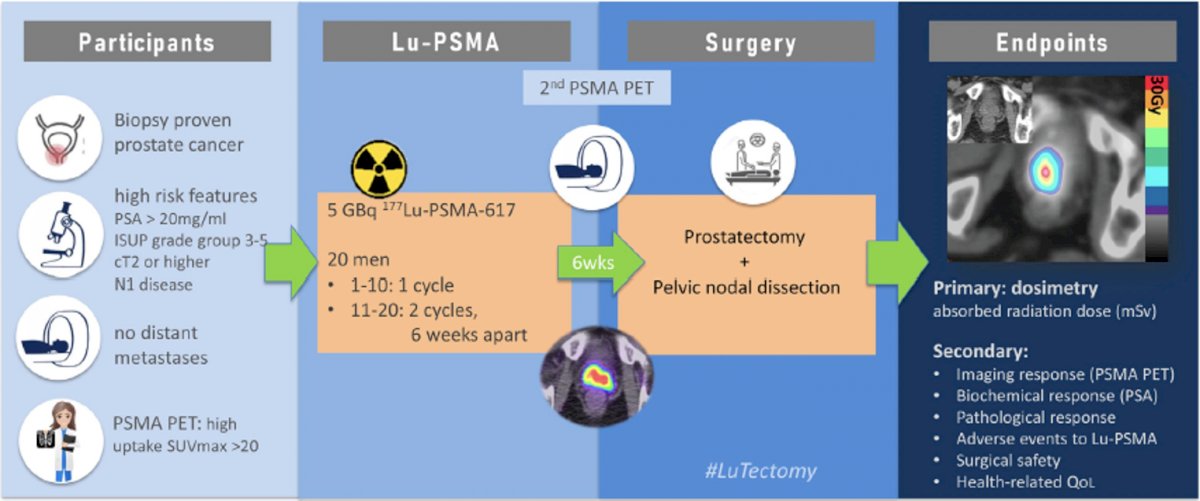
Preliminary data has shown that, among 10 patients, at least a partial response was observed in 60%, with 30% of patients having stable disease and only 1 (10%) having evidence of progression. Beyond these promising efficacy data, results to date suggest that this approach is safe without any evidence of grade 2 or greater adverse events attributable to the 177Lu-PSMA-617 and no grade 3 or greater surgical complications within 90 days. Observed adverse events were as expected with grade 1 dry mouth (xerostomia), fatigue, and nausea. Importantly, there was limited radiation dose to critical organs such as the parotid glands (2 Gy) and the kidneys (3 Gy). The authors noted that one patient’s surgery was slightly more difficult than expected but the remaining 9 had surgery as anticipated.
In terms of dosimetry, the authors found a median prostate dose of 48 Gy, though with wide confidence limits (less than 20 Gy to nearly 120 Gy). This resulted in approximately 80% decrease in PSA. However, interestingly, with this single treatment, no pathological complete responses or patients with minimal residual disease were identified. Thus, the ongoing cohort B of this trial will assess the potential benefit of adding a second cycle of therapy.
While most patients undergoing surgery do not receive neoadjuvant ADT, there is some suggestion that concomitant use of ADT with 177Lu-PSMA may enhance cancer killing. We know that the combination of ADT with external beam radiotherapy in high-risk disease improves survival compared to radiotherapy alone, likely as ADT potentiates radiation damage by inhibiting DNA damage repair.
Both xenograft mouse models and in vivo studies have demonstrated that testosterone suppression (i.e. with ADT or novel androgen receptor axis targeting agents such as enzalutamide) can induce a 1.5 to 2 fold increase in PSMA expression. To understand the effect of this on clinical outcomes, the Nautilus trial has been designed to assess the effect of ADT on PSMA expression and radiation dose delivery. Patients with high-risk or very high-risk prostate cancer undergoing radical prostatectomy will be randomized to receiving either 177Lu-PSMA for 2 cycles prior to surgery or 177Lu-PSMA with ADT. The trial aims to accrue 15 patients to each arm with a primary endpoint of dosimetry.
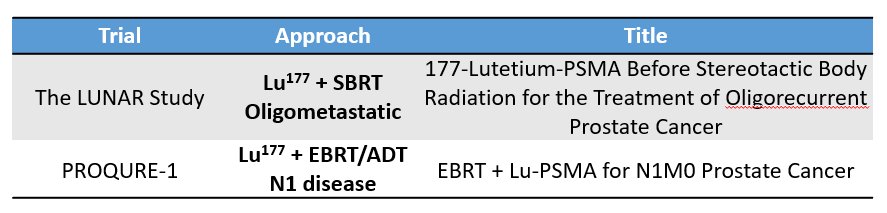
She emphasized that there is a logic for the complementarity of theranostics and external beam radiotherapy – external beam radiotherapy is spatially based while theranostics is biologically based. Thus, we may consider a paradigm of external beam radiotherapy to gross, radiologically visible disease with theranostic treatments for micrometastatic disease. A better understanding of theranostic dosimetry is critical to understanding radiobiology (both in tumor and normal tissue) and to understand safe combination approaches. A number of trials are assessing such combinations.
Thus, looking forward, she highlighted that there are many potential opportunities to integrate theranostic approaches in the high-risk localized prostate cancer disease space. Among patients undergoing surgery, we can consider neoadjuvant approaches, adjuvant treatment for those with high-risk features at the time of surgery, or this as salvage treatment. In the context of those undergoing radiotherapy, she emphasized that integration into the existing paradigms will likely be driven by an understanding of dosimetry as determined by the neoadjuvant prostatectomy studies. There is a further role in the adjuvant space for these patients as well.
While the data discussed so far (and most data in the metastatic space) have focused on 177Lu-PSMA, Dr. Hoffman noted that 225Ac may have some benefits in this patient population. The alpha particle emitted from 225Ac, compared to the beta particle from 177Lu, may more efficiently treat the small volume of disease present in micrometastatic deposits among these patients. Alpha particles have higher linear energy transfer which should provide a more effective cell kill (higher RBE). Additionally, the shorter range provides more local deposition of dose – while the range for a beta particle form 177Lu is 700 mM (approximately 20-25 cellular diameters), the range of an alpha particle from 225Ac is only 47 mM (approximately 1-2 cell diameters).
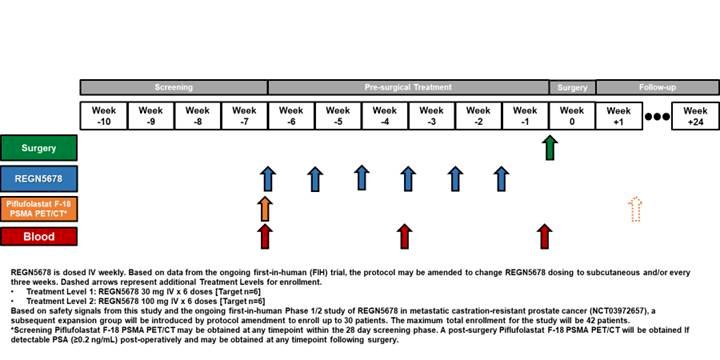
While this session of the SUO meeting has focused heavily on theranostics with targeted radioemitters, Dr. Hoffman also noted that other novel treatment paradigms are moving into the high-risk localized disease space. One such approach is the t-cell bispecific immunotherapy (BITEs). These agents bring T-cells into proximity with tumor cells and have shown clinical activity in prostate cancer. A neoadjuvant trial of this approach prior to radical prostatectomy is currently underway and attempting to enroll 47 patients for whom tumor tissue will be analysed for tumor response and immune analysis.
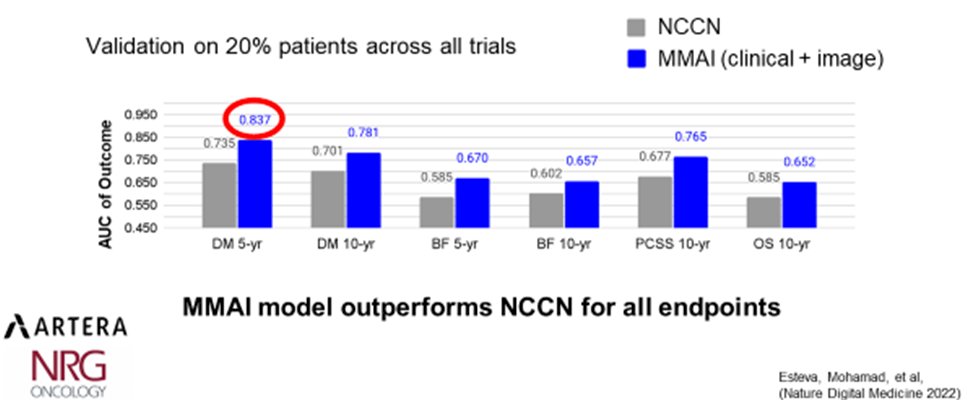
To contextualize all of these attempts to intensify therapy for patients with high-risk disease, Dr. Hoffman emphasized the importance of patient selection and personalization of care. Highlighting data published by Esteva and colleagues this year, she noted that the Artera MMAI mode outperforms standard risk prediction using NSSN criteria for prognostication of 5- and 10-year distant metastases, 5- and 10-year biochemical failure, 10-year cancer specific survival, and 10-year overall survival.
While there is clearly much work to be done in this space, she noted that treatment intensification with theranostics may actually allow de-intensification of other aspects of care. In particular, she noted the potential to reduce the durations of ADT co-administered with external beam radiotherapy in both the upfront definitive setting and in the salvage setting for recurrence following radical prostatectomy. Additionally, she suggested that theranostic treatment may be a suitable replacement for salvage radiotherapy for a subset of select men with biochemical recurrence following prostatectomy.
In conclusion, she highlighted that there is evidence that radiotherapy can address and treat microscopic disease in patients with high-risk prostate cancer, with a clinical benefit. Radiotherapy delivery using theranostic approaches may allow for further refinement of this treatment paradigm. However, ongoing and additional studies are needed to identify how to optimally integrate theranostics with existing local treatment approaches.
Presented by: Karen Elizabeth Hoffman, MD, MHSc, MPH, The University of Texas MD Anderson Cancer Center, Houston, TX