(UroToday.com) At the second Prostate Cancer Session of the Annual Meeting of the Society of Urologic Oncology, Dr. Mark Preston discussed the role of neoadjuvant therapy prior to radical prostatectomy.
He began by overviewing the epidemiology of prostate cancer: prostate cancer remains the solid tumor with the highest incidence among men (with an estimated 248,530 cases annually in the United States, representing 26% of all cancer diagnoses) and the second most common cause of cancer-related mortality (with an estimated 34,130 attributable deaths annually, representing 11% of all cancer-related deaths in the United States). From an annual cross-section to looking at this longitudinally, he noted that approximately 1 in 6 men will be diagnosed with prostate cancer though 60 to 70% of men will harbour disease (including those who never manifest clinically) and 3 to 4% of men will die from prostate cancer.
The vast preponderance, though somewhat shrinking in recent years, of men diagnosed with prostate cancer present with localized disease. Among those with localized disease, approximately 15% will have high-risk features based on their PSA, Gleason score and stage. These patients have increased risk of cancer-related death, with 15-year prostate cancer specific mortality that reaches nearly 40%. Dr. Preston highlighted that, as was shown in data from Dr. Eggener and colleagues more than 10 years ago now, these men have greater risks of cancer related mortality than other competing risks.
Thus, there is a pressing need to improve outcomes for these men. To highlight this, Dr. Preston presented the case of a 60 year old man presenting with a PSA of 9 and a palpable abnormality of digital rectal examination (cT2a). Subsequent prostate biopsy demonstrated Gleason score 4+4 disease in 4 of 12 samples cores. Using the MSKCC risk calculator (https://www.mskcc.org/nomograms/prostate/pre_op), he emphasized that this man will have a progression-free probability of 39% at 5 years and 26% at 10 years following radical prostatectomy. Thus, surgery alone is clearly insufficient. As a result, he noted that we need to improve outcomes for men with high-risk, locally advanced prostate cancer.
One way to do this is systemic therapy prior to surgery. This approach, with neoadjuvant androgen deprivation therapy (ADT), has been studied extensively in the past demonstrating improvements in positive surgical margins but no effect on biochemical recurrence or other more clinically meaningful outcomes. However, Dr. Preston noted that there are systematic limitations of these studies which dramatically affect their relevance to this question. First, these studies utilized standard LHRH agonists, with or without first-generation anti-androgens. Second, most of these studies enrolled patients with low risk disease, did not systematically evaluate pathologic response and lacked long-term follow-up.
Thus, with the advent of more potent androgen axis targeting agents with proven benefit in more advanced disease settings, there is an opportunity to re-evaluate this clinical paradigm. In particular, contemporary studies focus on those patients with high-risk disease, utilize modern systemic therapy approaches, integrate systematic central pathology review, and embed long-term clinical follow-up. Dr. Preston noted that the approaches being examined in these studies are substantially more effective than the treatment paradigms evaluated previously.
To contextualize these advances in prostate cancer, Dr. Preston noted that neoadjuvant therapy is the standard of care in many other tumor sites, including breast, rectal, and bladder cancers, on the basis of improved long-term survival. Further, this paradigm allows downstaging of the local disease which may facilitate surgical resection, may reduce or delay post-surgical therapies, and allows an in vivo assessment of the response to treatment that may allow subsequent escalation or de-escalation of therapy on the basis of this response.
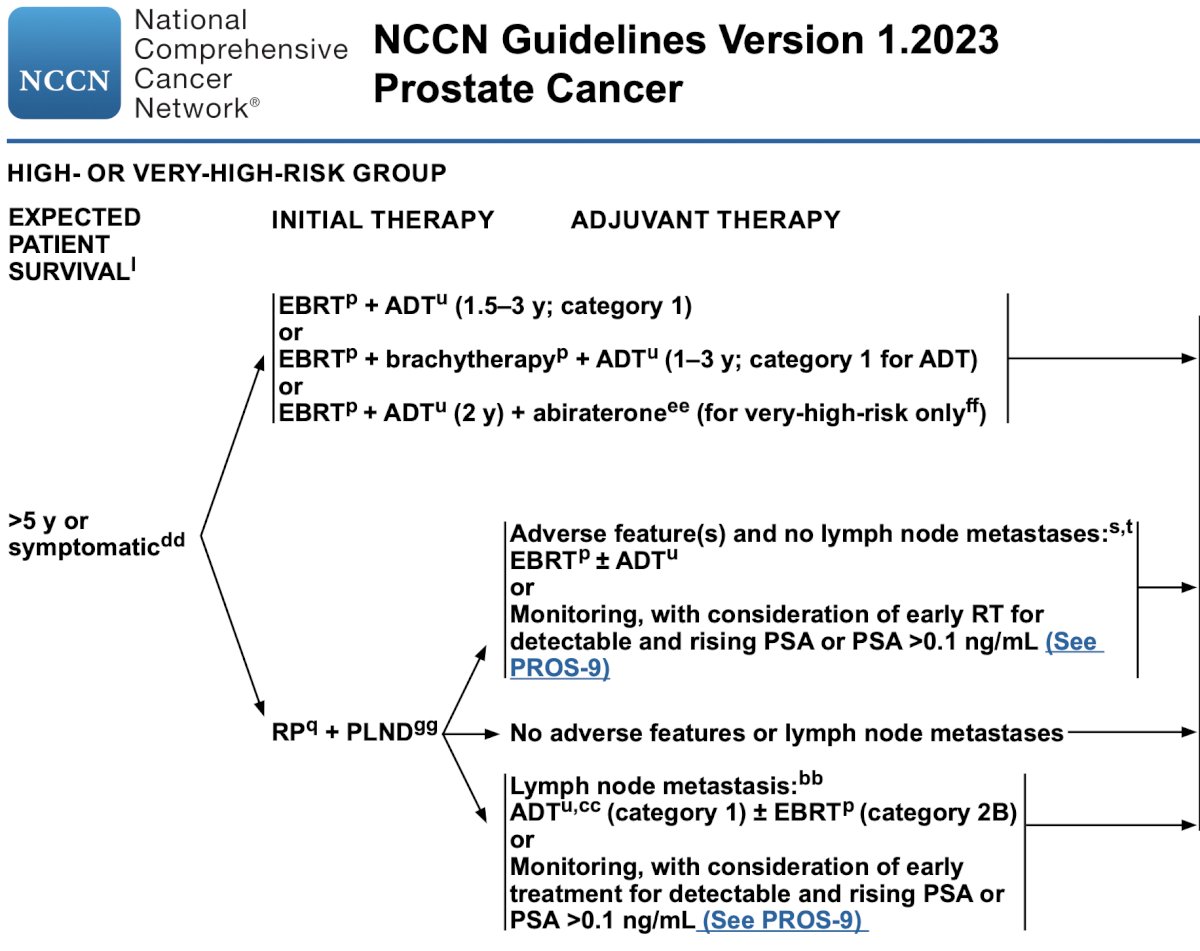
In the context of prostate cancer, he noted that the radiation oncology literature has shown us that local therapy alone is often inadequate in curing men with clinically-localized, high-risk prostate cancer. Indeed concomitant ADT before, during, and after radiotherapy has become the standard of care on the basis of improvements in disease-free and overall survival. The most recent version of the NCCN clinical practice guidelines for prostate cancer note that, in patients with very-high-risk disease, abiraterone may be added to external beam radiotherapy and ADT based on improved results seen in STAMPEDE, among patients with at least two of the following high-risk characteristics: cT3-4, Grade Group 4 or 5, or PSA >40 ng/mL.
Diving a little deeper into these data from STAMPEDE, Dr. Preston discussed the recent publication from Dr. Attard. These high-risk patients were randomized to either ADT alone or intensified therapy which may have included the addition of abiraterone or abiraterone and enzalutamide. While there wasn’t additional benefit from the combination of both agents, treatment intensification was associated with significant improvements in metastasis-free survival (from 69% to 82% at 6 years).
In the context of patients opting for surgery, there are numerous relevant questions including what pathologic outcomes men, can we decrease utilization of salvage therapies, to what extent does this result in overtreatment, is surgery after neoadjuvant therapy more difficult, can we identify those most likely to benefit, and, most importantly, does it improve long-term outcomes? Fundamentally, he posted the question about the risk of overtreatment given that we know salvage radiotherapy with ADT can be offered currently. To address these questions, he highlighted several phase 2 trials performed by the Boston group, assessing each of these with a variety of different treatment approaches.

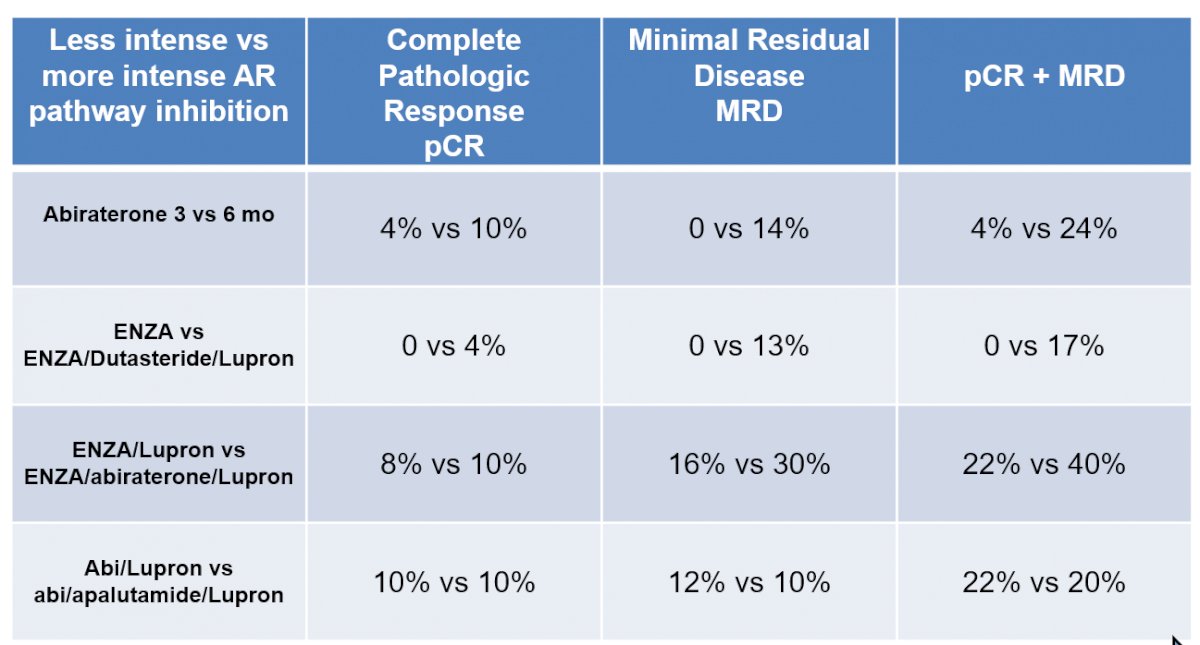
Taken together, there was evidence of higher pathological responses in patients who received intensified pre-operative systemic therapy.
Importantly, these early pathologic outcomes correlate with longer term clinical outcomes including biochemical recurrence. Among a cohort of patients with high-risk disease in which the overall 3-year biochemical recurrence-free survival was 59%, those who were non-responders had substantially lower rates (49%) than those who achieved a complete response or had minimal residual disease (95%).
In terms of the question of better identifying those patients who are likely to benefit, he noted work led by Dr. Rana McKay who identified that patients who were ERG mutation positive or have PTEN loss had significantly larger residual tumors following neoadjuvant therapy. Further, there were no patients with these genetic features who had minimal residual disease. Additionally, there appeared to be an additive effect with dual ERG positivity and PTEN-loss being associated with the highest residual tumor volume. Thus, these analyses suggest that tumors with these features have a resistance to intense androgen deprivation therapy. Similar findings were demonstrated in the recently published ARNEO trial among those with PTEN loss. In this randomized phase II trial, 89 patients were randomized to received with ADT along or with apalutamide prior to radical prostatectomy. The combination approach improved pathological responses with a minimal residual disease rate of 38% versus 9%, though those patients with PTEN loss were significantly less likely to have the minimal residual disease (11% vs 43%, p=0.002) and had a higher tumor burden at final pathology (1.6 vs 0.40 cm3, p<0.0001). As assessed with PSMA-PET imaging, there were impressive local tumor responses among those receiving intensified therapy with apalutamide.
Finally, Dr. Preston addressed the question of whether these paradigms can improve metastasis-free survival. To this end, he cited data from the CALBG 90203 trial in which 788 men were randomly assigned to receive neoadjuvant chemohormonal therapy for 18-24 weeks prior to radical prostatectomy. The primary study endpoint was biochemical progression-free survival at 3 years, though patients were followed for a median of 6.1 years. There was no significant difference seen in biochemical progression-free survival at 3 years (89% vs 84%). However, assessing secondary outcomes, neoadjuvant therapy was associated with improved overall biochemical progression-free survival (hazard ratio [HR], 0.69; 95% CI, 0.48 to 0.99), improved event-free survival, improved MFS (HR, 0.70; 95% CI, 0.51 to 0.95), and improved OS (HR, 0.61; 95% CI, 0.40 to 0.94) compared with RP alone. However, these benefits must be weighed against the toxicity of the approach, with grade 3 and 4 event rates during chemotherapy of 26% and 19%, respectively.
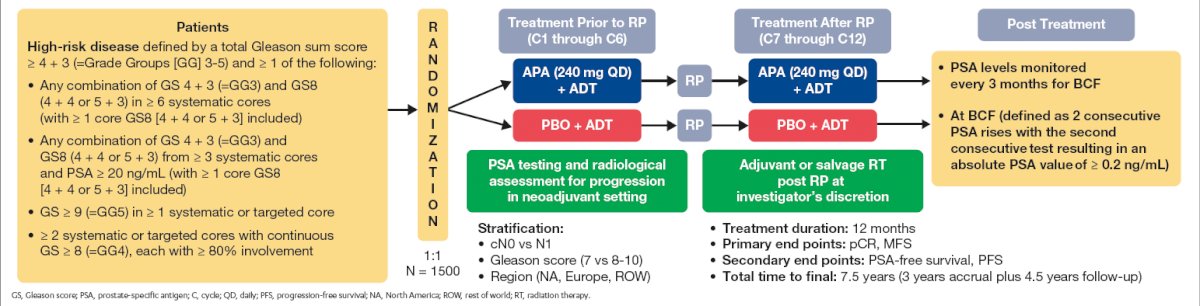
Given that advanced androgen inhibition has become the standard of care for patients with advanced prostate cancer, randomized phase 3, double-blind trials are assessing these approaches in High-risk, Localized, or Locally Advanced Prostate Cancer. One such trial is PROTEUS (https://clinicaltrials.gov/ct2/show/NCT03767244) which is evaluating apalutamide along with ADT in this space. This trial completed the accrual of 2170 patients in June of 2022. The last on-protocol prostatectomy will be performed in December 2022 and pathology results will likely be available as soon as the end of 2023. Data regarding metastasis-free survival are expected in 2026 or 2027.
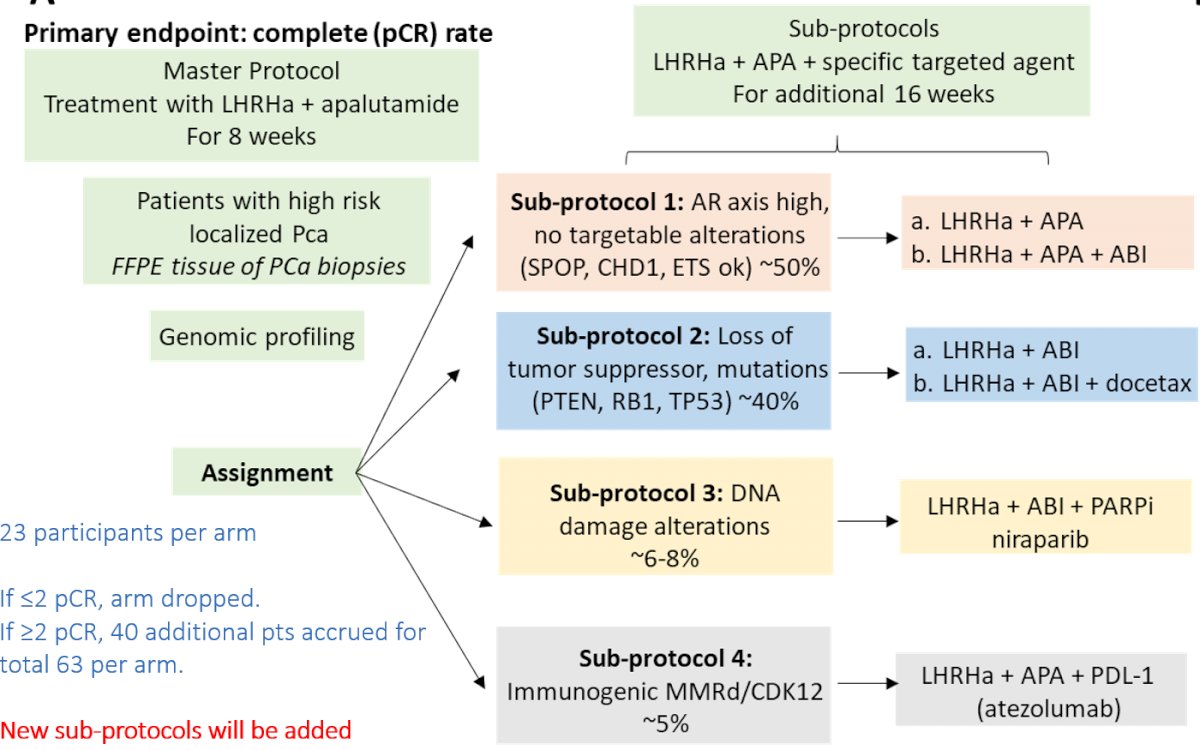
There are further sub-studies of PROTEUS utilizing both PSMA and conventional imaging to follow patients through until the development of metastatic disease. To further personalize care, Dr. Preston noted that the GUNS trial is providing biomarker-driven neoadjuvant therapy on the basis of genomic profiling results with a primary endpoint of pathological complete response.
In conclusion, Dr. Preston noted the pressing need to improve outcomes for men with localized high-risk prostate cancer. Contemporary neoadjuvant approaches show promise though phase III data are needed to show benefit in terms of clinically relevant endpoints such as metastasis-free survival.
Presented by: Mark A. Preston, MD, MPH, Brigham and Women's Faulkner Hospital, Division of Urology, Jamaica Plain, MA