(UroToday.com) The 2022 SUO annual meeting featured the Huggins Medal Lecture, with this year’s recipient Dr. Harry Herr discussing neoadjuvant chemotherapy and bladder sparing surgery for muscle invasive bladder cancer. Prior to starting his presentation, Dr. Herr took time to recognize six key mentors and friends that significantly impacted his career:
- Lloyd Old: the father of modern tumor immunology, who’s lab Dr. Herr worked in for 2 years
- Willet Whitmore, Jr: the father of urologic oncology, who developed the first organized urologic oncology training program in the United States. Dr. Herr was Dr. Whitmore’s first 2-year fellow when this program started
- Alan Yagoda: medical oncologist and early proponent of chemotherapy in the treatment of bladder cancer
- Pram Sogani: urologic oncologist at Memorial Sloan Kettering Cancer Center for nearly 50 years
- Myron Melamed: one of the key early genitourinary pathologists
- Victor Reuter: world renowned genitourinary pathologist
Dr. Herr also acknowledged the many urologic oncology fellows that he had a hand in training during his career at Memorial Hospital, the majority of which are leaders in the urologic oncology world today:
Dr. Herr started by emphasizing that bladder preservation has rewards, risks and requirements. Indeed, the bladder is an organ that can be and is worth saving: we can live without a bladder, but its presence represents a cancer risk. Thus, bladder-sparing is justified only if we can detect and salvage failures, with the goals of preservation being: local disease control, maintaining a functioning bladder, and preserving overall survival. Based on historical autopsy studies from Dr. Hugh Jewett, Dr. Herr notes that some invasive cancers have no nodal or distant metastases. These include tumors confined to the muscle (not through the bladder wall), solitary (small), and with no ureteral obstruction.
Neoadjuvant chemotherapy is the treatment of micrometastases, which is the ultimate cause of death from invasive disease. As such, this is an important and part of an integrated approach aimed at bladder preservation. MVAC was first introduced by Dr. Yagoda in 1983 and the first neoadjuvant chemotherapy trials began at Memorial Sloan Kettering Cancer Center in 1985. In 1998, Dr. Herr and colleagues published their 10-year outcomes of patients with invasive (T2-3N0M0) bladder cancer who responded completely to MVAC chemotherapy followed by bladder-sparing surgery.1 Among 111 surgical candidates, 60 (54%) achieved a complete clinical response (T0) on transurethral resection of the primary tumor site. Of these, 28 requested follow-up with TUR alone, 15 had a partial cystectomy, and 17 elected a radical cystectomy. These patients were followed up for a median of 10 years (range, 8 to 13 years). Overall, among the 43 patients who had bladder-sparing surgery, 32 (74%) were alive, including 25 (58%) with an intact functioning bladder. Twenty-four patients (56%) developed bladder tumor recurrences from 5 to 96 months, which were invasive in 13 (30%) and superficial in 11 (26%). Ultimately, 13 patients required a salvage cystectomy, of whom 6 died, including 4 (9%) from a new invasive neoplasm. Of the 17 patients who had radical cystectomy, 11 (65%) were alive at the time of last study follow-up.
Dr. Herr then presented a case presentation of a 62 year old healthy male physician who was diagnosed with a cT2 single 4 cm tumor on the left posterior bladder wall. He had a complete transurethral resection, which demonstrated urothelial carcinoma with squamous features. There was no mass on examination under anesthesia, no hydronephrosis, and no adenopathy:
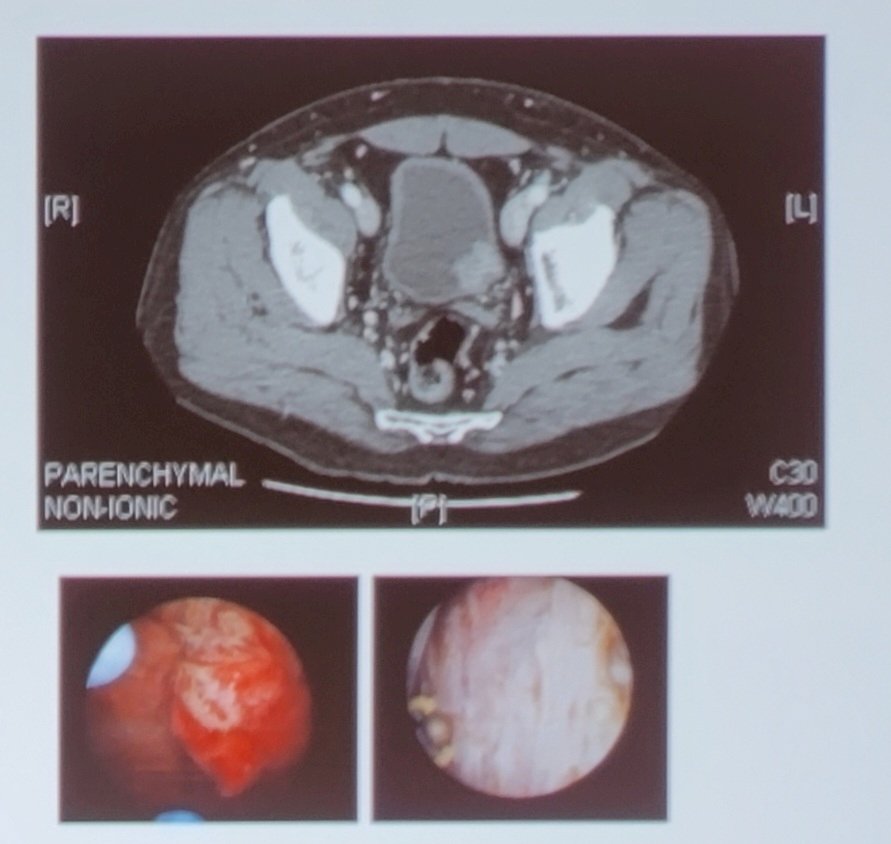
Given his excellent eGFR of 74, he was treated with 4 cycles of MVAC, had a post-chemotherapy transurethral resection that showed no residual disease, and he is now alive and functioning with an intact bladder for 20 years.
Dr. Herr then discussed data over 20 years in his practice at Memorial Sloan Kettering Cancer Center, which includes 191 patients undergoing bladder sparing surgery. These patients had the following criteria: cT2N0M0, solitary, <5 cm, and a transurethral resection x2. They were subsequently treated with 3-6 cycles of cisplatin-based neoadjuvant chemotherapy followed by a post-chemotherapy transurethral resection (cT0) and a negative CT/MRI. Overall, bladder sparing surgery was feasible in 160 patients (31 patients ultimately undergoing a radical cystectomy), including 97 patients undergoing TURBT + surveillance and 63 patients undergoing partial cystectomy. The patient characteristics of these 160 patients is as follows:

The patients undergoing partial cystectomy, these patients all undergo a pelvic lymph node dissection, with the ureter being reimplanted in 28% of cases. Comparing those patients that underwent bladder sparing surgery (n = 160) to those undergoing radical cystectomy (n = 31), the overall survival rates were 63% and 64%, respectively:

Among the patients undergoing bladder sparing surgery, 144 patients (90%) have no evidence of disease, and 16 patients (10%) died of disease. Furthermore, 130 patients are alive with a bladder (82%) and 14 patients have no evidence of disease after salvage radical cystectomy. There have been 57 patients (37%) that had bladder recurrence, with a median time to recurrence of 3.3 years (range 15 months – 13 years):

Additionally, Dr. Herr notes that variant histology does not automatically preclude patients from considering bladder sparing surgery, given comparable cancer specific survival rates stratified by urothelial carcinoma only vs urothelial carcinoma + variant histology:

Dr. Herr emphasized that understaging the response to neoadjuvant chemotherapy is secondary to poor patient selection and quality of the transurethral resection. Among the 63 patients undergoing partial cystectomy, 93% had ypT0/TisN0, 1% had ypT0N+, 3% had ypT3N0, and 1% had ypT3N+ disease.
Dr. Herr concluded his presentation discussing neoadjuvant chemotherapy and bladder sparing surgery for muscle invasive bladder cancer with the following take home messages:
- Bladder sparing surgery is an option in appropriately selected, well-informed and compliant patients with non-metastatic, organ confined muscle-invasive bladder cancer
- Selection criteria is stringent, much more so than for trimodal therapy
- Comparable overall survival and disease-specific survival rates to radical cystectomy are attainable
- Bladder relapses occur in 1/3 patients, but with muscle invasive bladder cancer in only 10% of cases
- Excess mortality rates are ~8% and may be as high as 10%, thus the question remains: is an 8-10% excess mortality risk worth saving the bladder for 10+ years?
- Radiotherapy is not necessary in all muscle invasive bladder cancer cases to preserve the bladder, thus representing de-escalation of treatment
Dr. Herr concluded by thanking his wife, urologic oncologist Dr. Machele Donat.
Presented by: Harry Herr, MD, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 23rd Annual Meeting of the Society of Urologic Oncology (SUO), Nov 30 – Dec 2, 2022. San Diego, CA
References:
- Herr H, Bajorin DF, Scher HI. Neoadjuvant Chemotherapy and Bladder-Sparing Surgery for Invasive Bladder Cancer: Ten-Year Outcome. J Clin Oncol. 1998;16:1298-1301.