(UroToday.com) The Society of Urologic Oncology (SUO) 2021 annual meeting in Orlando, FL was host to an excellent, thought-provoking presentation by Dr. Jean Hoffman-Censits, MD, discussing whether there is evidence to justify extrapolating the benefit of neoadjuvant chemotherapy from bladder cancer to upper tract urothelial carcinoma (UTUC).
Current challenges in UTUC include:
- Scant biopsy samples that make preoperative clinical staging difficult compared to urothelial bladder cancer.
- Patient comorbidities that can raise concern for platinum tolerability (e.g. chronic kidney disease, neuropathy, etc.)
- Small study populations with little prospective data that makes risk/benefit discussions difficult
As demonstrated by Shiga et al.,1 upstaging of clinically non-muscle invasive UTUC to pT2 disease or worse occurs in greater than 30% of cases (15% to pT3 or worse). Although there is phase 3 data supporting post-operative chemotherapy in this disease space, renal function often declines following radical nephroureterectomy, precluding cisplatin-based chemotherapy regimens with cisplatin eligibility decreasing from 58% to 15% post-operatively.
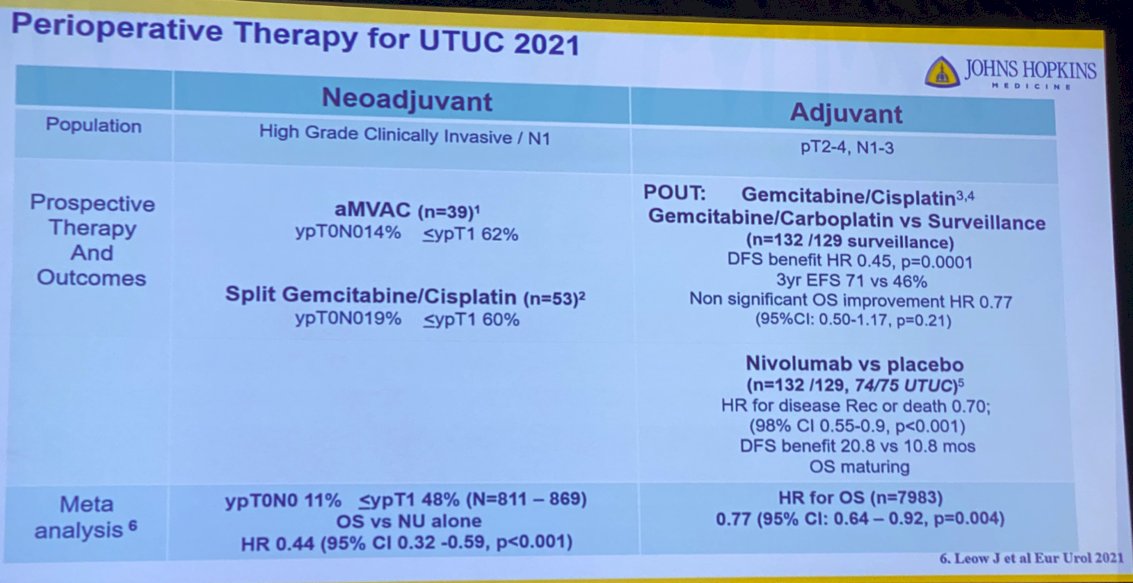
In the neoadjuvant space, there are currently two published studies evaluating chemotherapy regimens for high-grade clinically invasive/node-positive UTUC patients. Margulis et al. evaluated accelerated methotrexate, vinblastine, doxorubicin, and cisplatin (aMVAC) regimen in 39 patients with ypT0N0 rates of 14% and rates of ypT1 disease or less than 62%. A split gemcitabine/cisplatin regimen in 53 patients achieved corresponding rates of 19% and 60%, respectively.
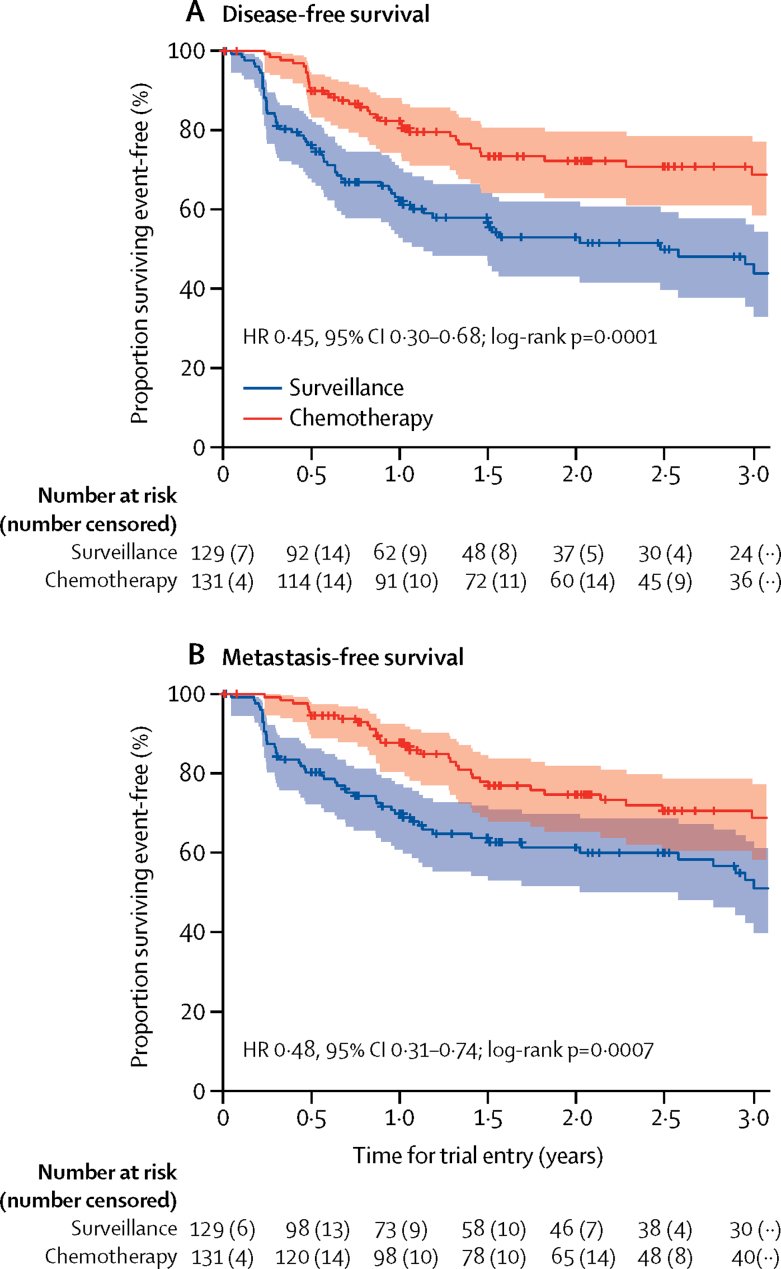
In the adjuvant space, the POUT trial has recently evaluated adjuvant gemcitabine/cisplatin or gemcitabine/carboplatin in cisplatin-ineligible patients compared to surveillance in ypT2-4, TanyN1-3 UTUC patients. This trial demonstrated a disease-free survival (DFS) benefit with HR of 0.45 (p=0.001) and 3-year event-free survival of 71% (intervention arm) versus 46% (surveillance arm). Overall survival was non-significantly improved (HR 0.77, 95% CI: 0.50-1.17, p=0.21).2
Dr. Hoffman-Censits went on to present data from CheckMate-274 that evaluated adjuvant nivolumab 240 mg intravenously every two weeks for up to one year versus placebo in patients with muscle-invasive urothelial carcinoma. This was a positive trial with median DFS improving from 10.8 to 20.8 months in the nivolumab arm.3
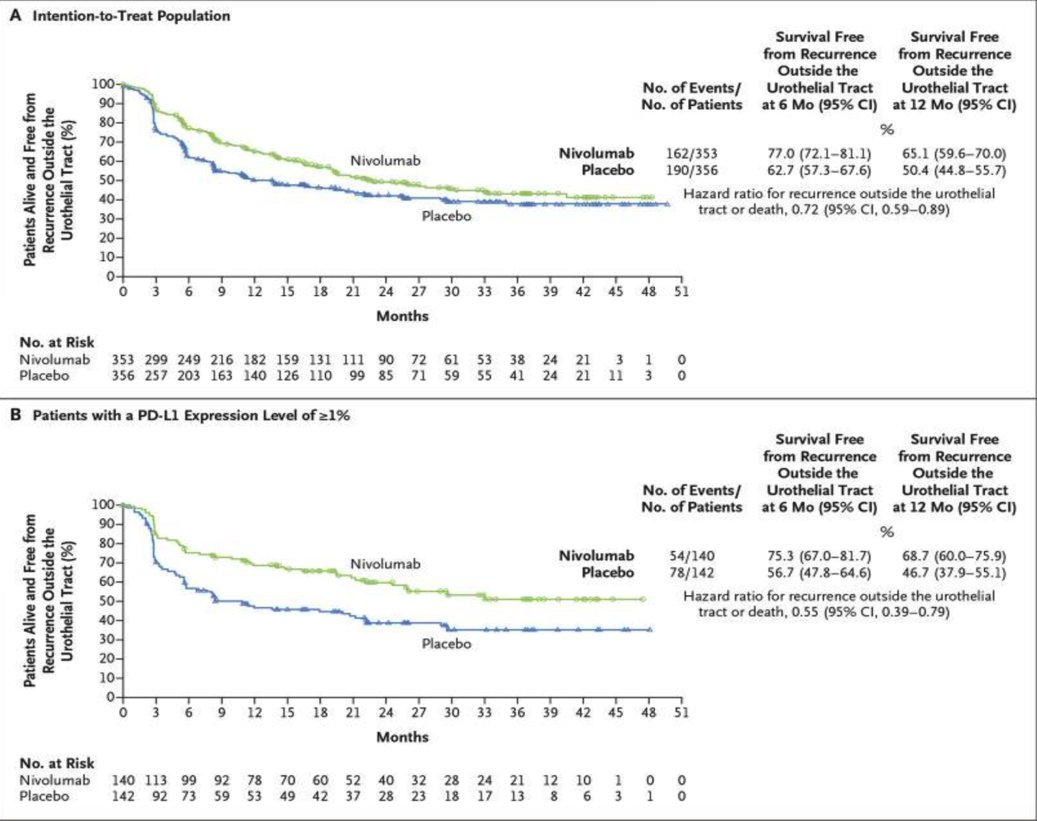
The question thus becomes whether this data can be generalized to patients with UTUC. This trial included 44 patients (12.5%) with disease originating from the renal pelvis and 30 (8.5%) with disease from the ureter in the intervention arm, compared to 52 (14.6%) and 23 (6.5%), respectively in the control arm. On subgroup analysis, the forest plot below demonstrates that this OS benefit does not translate to the subcohort of patients with renal pelvis or ureter tumors.

At this point, Dr. Hoffman-Censits revisited her initial question of why do we extrapolate the benefit of neoadjuvant chemotherapy from the bladder cancer to UTUC disease space?
- Chemotherapy is clearly active in UTUC
- Chemotherapy may no longer be feasible postoperatively due to renal function decline
- Upstaging makes treatment at earlier states compelling
- Chemotherapy sensitivity information based on final pathologic stage and adjuvant checkpoint choice (or trial) for non-responding patients
- Modest prospective data in the neoadjuvant setting
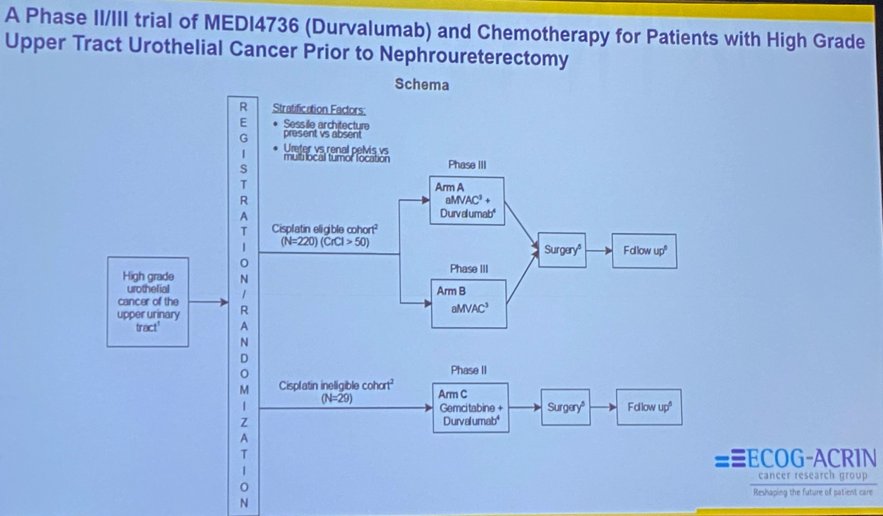
Dr. Hoffman-Censits went on to share a slide of ongoing and future trials of preoperative therapy in UTUC, highlighting NCT04628767, a phase II/III trial of MEDI4736 (Durvalumab) and chemotherapy for patients with high-grade UTUC prior to nephroureterectomy and shared a slide update of phase III adjuvant studies including UTUC.


In summary, Dr. Hoffman-Censits concluded that:
- POUT investigators have demonstrated that UTUC is a unique disease entity where prospective trials with meaningful practice changing clinical endpoints can lead to discovery and drug development - and not just a subgroup.
- Chemotherapy in the adjuvant setting exposes highest risk patients to a scenario whether they are least likely to complete a cisplatin course using cross trial comparison.
- Bladder neoadjuvant chemotherapy is superior to adjuvant chemotherapy - OS benefit, mounting retrospective and prospective UTUC data showing the same.
- Upstaging rate in UTUC is high.
- Biologic information regarding chemotherapy sensitivity and now adjuvant checkpoint choice (or trial) for non-responding patients is necessary.
- Trials are vital (URANUS, EA8192) to move extrapolation to evidence.
Presented by: Jean Hoffman-Censits, MD, Assistant Professor of Oncology, Johns Hopkins Greenberg Bladder Cancer Institute, Baltimore, MD
Written by: Rashid Sayyid, MD, MSc – Urology Chief Resident, Augusta University/Medical College of Georgia, @rksayyid on Twitter during the 2021 Society of Urologic Oncology (SUO) Winter Annual Meeting, Orlando, FL, Wed, Dec 1 – Fri, Dec 3, 2021.
References:
- Shiga M, Nagumo Y, Chihara I, et al. Discrepancy between clinical and pathological T stages in upper urinary tract urothelial carcinoma: Analysis of the Hospital-Based Cancer Registry data in Japan. Int J Urol. 2021 Aug;28(8):814-819.
- Birtle A, Johnson M, Chester J, et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): A phase 3, open-label, randomized controlled trial. Lancet 2020 Apr 18;395(10232):1268-1277.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021 Jun 3;384(22):2102-2114.