(UroToday.com) The Society of Urologic Oncology (SUO) 2021 annual meeting in Orlando, FL hosted the 2021 European Association of Urology (EAU) Annual Lecture. Dr. Michael Cookson graciously presented Dr. Maria Carmen Mir, MD, PhD, FEBU as the invited guest speaker and emphasized the importance of the SUO EAU Exchange Lectureship Program that serves to strengthen the relationship between the two societies and facilitates collaborations between European and American physicians.
Dr. Mir began her talk by highlighting several important facets/achievements of the EUA:
- Includes greater than 19,000 members across the globe
- Publishes the EAU guidelines in 30+ languages with 75 endorsements of national urological and other scientific organizations
- Publishes multiple peer-reviewed, indexed journals (European Urology, European Urology Focus, European Urology Oncology, and European Urology Open Science).
- Provides patient educational material (leaflets and animated videos) for 26 topics in 20 languages
- Created the EAU Patient Advocacy Group (EPAG)
- Creates educational online platforms (UROONCO and UROLUTS)
- Supports numerous collaborative research projects with a current network of 600+ research centers
- Engages in knowledge sharing with over 40 participants in the European Urology Scholarship Programme
- Promotes resident training via the European Urology Residents Education Programme
- Hosts educational events and meetings with over 20 courses across the globe
- Hosts the annual EAU Congress over five days with 144 sessions and 52,000 live attendees
Dr. Mir commenced the scientific portion of her talk by acknowledging that definitive pathologic reports remain the gold standard. However, she believes that real-time pathology reports are ready for prime time. She proceeded to introduce confocal laser microscopy (CLM) and explain how it works.
- CLM is based on tissue illumination with a low-power laser. The laser light is reflected from the tissue and refocused on the detection system by the same lens.
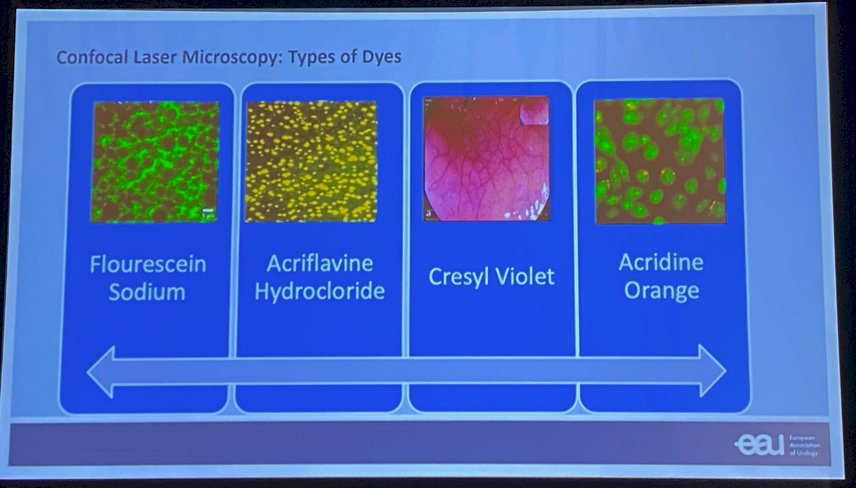
- To obtain confocal images, exogenous fluorescence agents have to be applied, which can be administered systemically or topically (see image below).
- CLM allows analysis of fluorescent labelled thick specimens without physical sectioning, generating a 3D reconstruction of images.
- Because images are detected by a computer, rather than the human eye, more color shades can be recognized.
- CLM provides high-resolution images, enabling optical biopsies and in vivo histology.
- CLM can be used on both live and fixed cells.
Dr. Mir next went on to introduce CLM endomicroscopy (CLE). CLE provides high-resolution images, enabling optical biopsies and, thus, in-vivo histologies. There are currently two available CLEs:
- Integrated endoscope system (Pentax ®)
- Probe-based system (Cellvizio ®)
The integrated system consists of conventional white light video endoscopes in which a confocal fluorescence microscope is integrated into the distal tip. Conversely, the probe-based CLE system (Cellvizio ®) represents a stand-alone confocal probe capable of being passed through the working channel of a standard video endoscope. CLE has been widely adopted in other medical disciplines including Gastroenterology (e.g. Barrett’s Esophagus) and Pulmonology. In Urology, CLE has been used to assess for potential positive surgical margins during robotic-assisted radical prostatectomies, identification of neurovascular bundles, and to evaluate prostate glands ex-vivo. Notably, CLE has been most prominently utilized in the upper tract urothelial cancer (UTUC) disease space, whereby this modality assists in real-time differentiation of normal tissue from both low- and high-grade cancer. This tool thus assists physicians in characterization of upper tract lesions during ureteroscopy and improves the diagnostic/treatment tools for quick decision making.

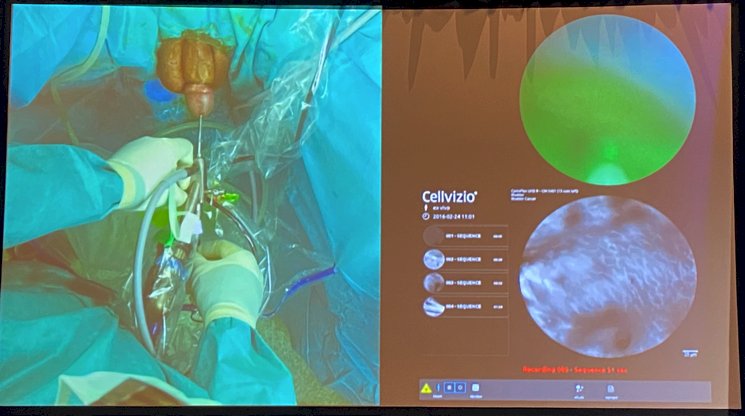
Dr. Mir went on to present an instructional video for Cellvizio ® utilization during ureteroscopy for upper tract disease that demonstrates the technique for instillation of the fluorescent agent through the ureteroscope and subsequent introduction/utilization of the Cellvizio ® probe through the working channel.

Accordingly, the EAU guidelines have acknowledged the potential role for Cellvizio ® during ureteroscopy for upper tract lesions with the following statement: “Optical coherence tomography and confocal laser endomicroscopy (Cellvizio ®) have been used in vivo to evaluate tumour grade and/or for staging purposes, with a promising correlation with definitive histology in high-grade UTUC”.
Dr. Mir went on to present data by Breda et al. that evaluated CLE’s utility for the real-time characterization of UTUC. Flexible ureteroscopies were performed in 14 patients with computed tomography (CT)-intravenous urography detected upper tract lesions (mean diameter 26 mm). Correspondence between the CLE images and the final histopathologic results was found in seven of seven (100%) cases of low-grade UTUC, five of six (83.3%) cases of high-grade UTUC, and one of one (100%) case of carcinoma-in-situ (CIS). An interobserver agreement k score=0.64 was observed between CLE and histological readings.1 Dr. Mir went on to highlight the strengths and limitations of this approach/study.
- Strengths:
- Improved characterization of lesions
- Real-time digital pathology
- Limitations:
- Lack of radical nephroureterectomy correlation
- Low number of included patients
- Surgeon-dependent learning curve
- Bias secondary to prior CT and urinary cytology results
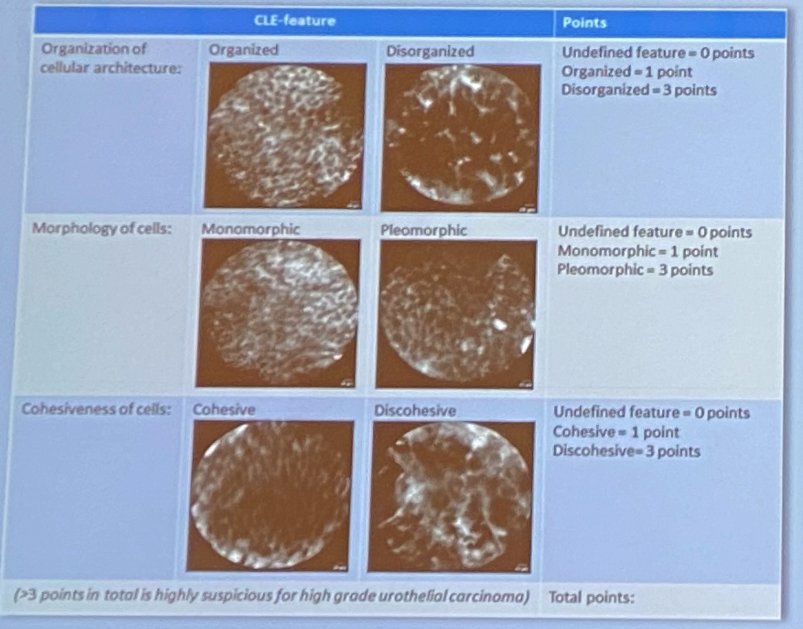
Freund et al. have since developed a Cellvizio ® scoring system that allows for real-time tumor grading based on: (i) organization of cellular architecture, (ii) cellular morphology, and (iii) cell cohesiveness. Zero, one, or three points are assigned to each domain and a total score of greater than three predicted a high likelihood of high grade urothelial carcinoma.2 The same group subsequently validated three histologic features as the most prominent ones to differentiate low from high-grade UTUC:3
- Cellular organisation (organised versus disorganised)
- Morphology (Monomorphic versus pleomorphic)
- Borders (Distinct versus indistinct)
There have been numerous reports regarding the utilization of in-vivo CLM in the prostate cancer space with all significant attempts limited by: (i) black and white images or images with a particular color-coding scheme, (ii) images differing from those analyzed by pathologists, (iii) steep learning curve, and (iv) lengthy prep time.
Dr. Mir next presented the ex-vivo, point-of-care fluorescence CLM: VIVASCOPE 2500-G4 (MAVIG ®) that has been available since 2001. This modality requires one mm width of tissue and utilizes Orange Acridine dye. This modality was initially applied in the Dermatology discipline, specifically during Mohs surgery. Lessons learned from our Dermatology colleagues’ experiences included:
- Real-time tissue evaluation
- Ability to identify non-diagnostic biopsies→ immediately perform repeat biopsies
- Immediately informs treatment due to high correlation with final pathologic diagnosis
- Has no detrimental effect on tissue for formal pathology review
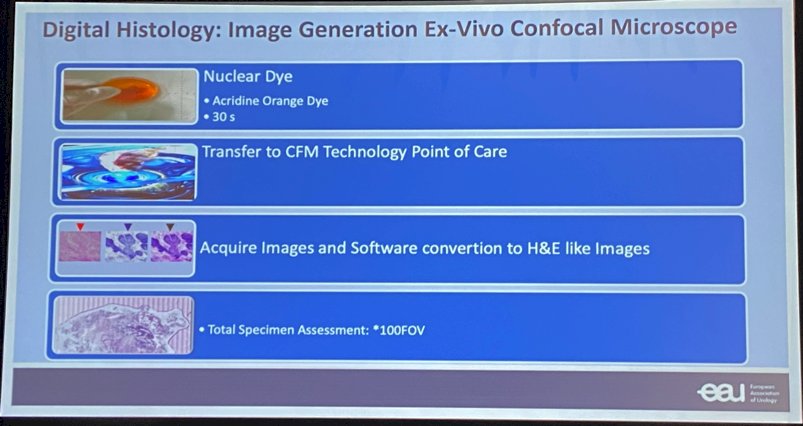
Dr. Mir went on to illustrate how digital histology images are obtained using ex-vivo confocal microscopes (see image below).
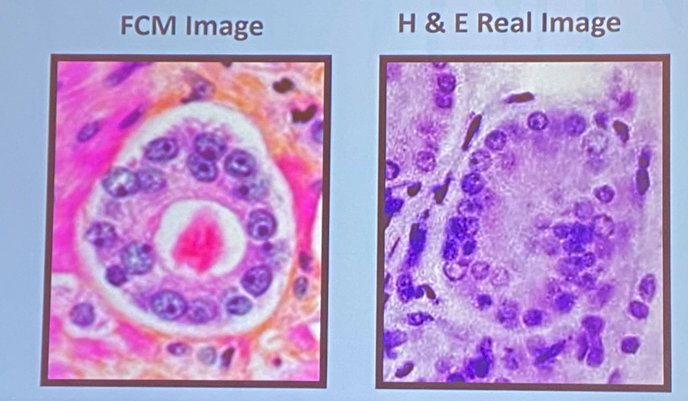
Fluorescence CLM has been utilized in the prostate cancer disease space to differentiate between positive and negative prostate biopsy cores. A study by Rocco et al. evaluated the diagnostic utility of fluorescence CLM for prostate cancer identification and grading, compared to Hematoxylin-Eosin (HE) stains. Utilizing 427 slides for each technique from 54 patients, the authors demonstrated a comparative prostate cancer detection rate that was almost perfectly correlated with a 95.1% correct diagnosis rate using fluorescence CLM and a k score=0.84. The inter-rater agreement for cancer grade attribution was lower at k=0.47.4 Similar work by Marenco et al. demonstrated a histopathological evaluation agreement k score=0.81 at the prostate biopsy level and 0.69 at the region of interest level. The corresponding positive and negative predictive values were 85% and 95% at the biopsy core level and 84% and 86% at the region of interest level.5 Rocco et al. subsequently evaluated fluorescence CLM in radical prostatectomy frozen sections. Surgical margin evaluation was deemed feasible using this technique. There was a 94-97% level of agreement between fluorescence CLM and HE stains for the accurate detection of muscle, nerves, vessels, and fatty tissue.6 This group subsequently performed a prospective analysis of 24 patients undergoing robotic radical prostatectomies with intraoperative fluorescence CLM for positive surgical margin (PSM) evaluation using the Mohs shaving technique. The primary endpoint was PSM at the neurovascular bundle. Four PSMs were detected and re-resected with all of them eventually having negative margins.7
This real-time tissue diagnostic approach also has implications with regards to focal therapy, whereby sample biopsies can be obtained and evaluated in real-time to ensure that the ablative region has not missed active disease. This approach also has utility for small renal mass biopsy cores to minimize the rate of non-diagnostic procedures.
Dr. Mir concluded with the following take-home messages:
- CLE aims to assists surgeons in intraoperative assessment of UTUC
- Fluorescent CLM provides fast, real-time digital accurate pathology diagnosis that might facilitate treatment decision making
- Teamwork between pathologists and urologists is mandatory for correct interpretation of images
- Advantages: fast, reproducible
- Disadvantages: the learning curve
- Requires further validation and standardization
Presented by: Dr. Maria Carmen Mir, MD, PhD, FEBU, Department of Urology, Fundacion Instituto Valenciano Oncologia, Valencia, Spain
Written by: Rashid Sayyid, MD, MSc – Urology Chief Resident, Augusta University/Medical College of Georgia, @rksayyid on Twitter during the 2021 Society of Urologic Oncology (SUO) Winter Annual Meeting, Orlando, FL, Wed, Dec 1 – Fri, Dec 3, 2021.
References:
- Bred A, Territo A, Guttilla A, et al. Correlation Between Confocal Laser Endomicroscopy (Cellvizio ®) and Histological Grading of Upper Tract Urothelial Carcinoma: A Step Forward for a Better Selection of Patients Suitable for Conservative Management. Eur Urol Focus. 2018 Dec;4(6):954-959.
- Freund JE, Liem EIML, Savci-Heijink CD, et al. Confocal laser endomicroscopy for upper tract urothelial carcinoma: validation of the proposed criteria and proposal of a scoring system for real-time tumor grading. World J Urol. 2019 Oct;37(10):2155-2164.
- Liem EIML, Freund JE, Savci-Heijink CD, et al. Validation of Confocal Laser Endomicroscopy Features of Bladder Cancer: The Next Step Towards Real-time Histologic Grading. Eur Urol Focus. 2020 Jan;6(1):81-87.
- Rocco B, Sighinolfi MC, Sandri M, et al. Digital Biopsy with Fluorescence Confocal Microscope for Effective Real-time Diagnosis of Prostate Cancer: A Prospective, Comparative Study. Eur Urol Oncol. 2021 Oct;4(5):784-791.
- Marenco J, Calatrava A, Casanova J. Evaluation of Fluorescent Confocal Microscopy for Intraoperative Analysis of Prostate Biopsy Cores. Eur Urol Focus. 2020 Sep;S2405-4569(20)30255-8.
- Rocco B, Sighinolfi MC, Cimadamore A, et al. Digital frozen section of the prostate surface during radical prostatectomy: a novel approach to evaluate surgical margins. BJU Int. 2020 Sep;126(3):336-338.
- Rocco B, Sarchi L, Assumma S, et al. Digital Frozen Sections with Fluorescence Confocal Microscopy During Robot-assisted Radical Prostatectomy: Surgical Technique. Eur Urol. 2021 Dec:80(6):724-729.