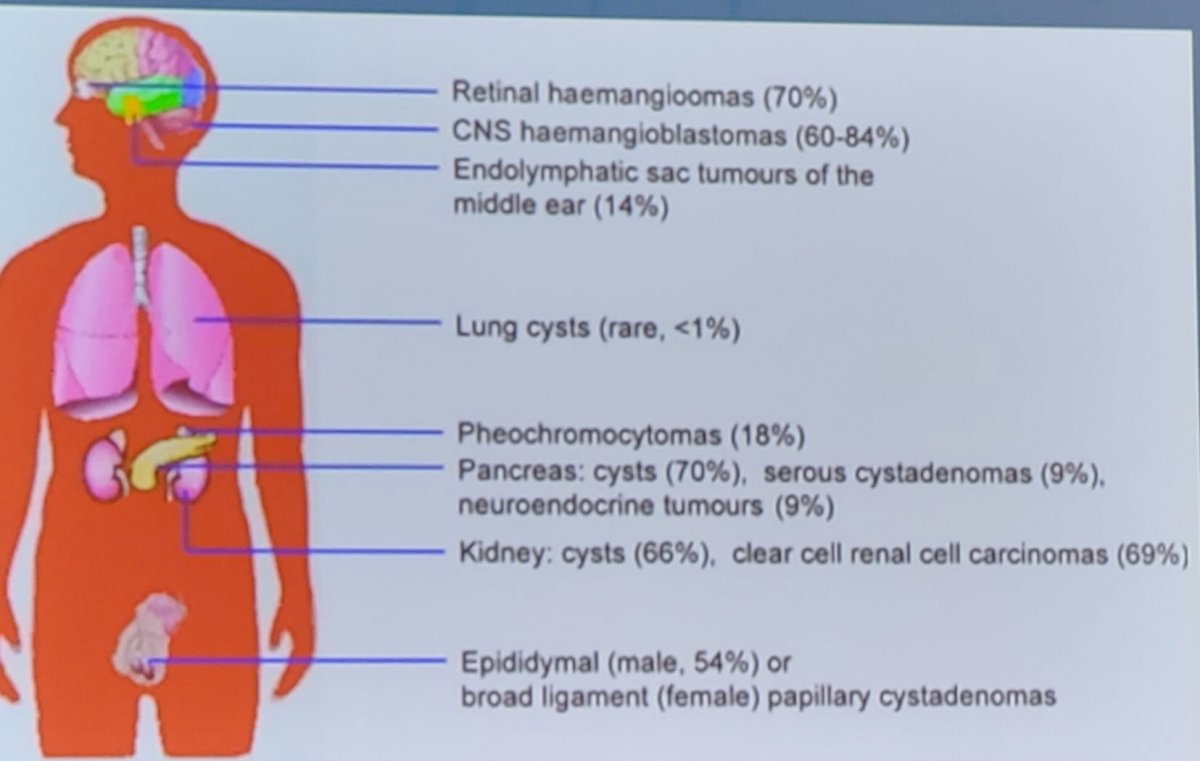
(UroToday.com) The Society of Urologic Oncology (SUO) annual winter meeting included a kidney cancer session and a presentation by Dr. Jodi Maranchie discussing targeting HIF-2alpha in von-Hippel Lindau (VHL) patients. Dr. Maranchie starts by noting that the manifestations and penetrance of VHL lesions are highly variable based on anatomic location:
Two decades ago, Dr. Maranchie’s group performed seminal work assessing the contribution of VHL substrate binding and HIF1-alpha to the phenotype of VHL loss in RCC.1 In this study, they demonstrated that competitive inhibition of the VHL substrate recognition site with a peptide derived from the oxygen degradation domain of HIF1alpha recapitulates the tumorigenic phenotype of VHL-deficient tumor cells. Specific to HIF-2alpha inhibitors, these allosterically prevent binding to the HIF-1beta subunit with no effect on HIF-1alpha. Additionally, HIF-2alpha inhibitors prevent DNA binding and HIF-2alpha transactivation of downstream targets and thus suppress tumor growth.
The mechanistic work delineating HIF-2alpha inhibition over the last several years lead to the NCT03401788 trial assessing MK-6482 (Belzutifan) in patients with VHL, recently published in the New England Journal of Medicine.2 The study schema for this trial is as follows:
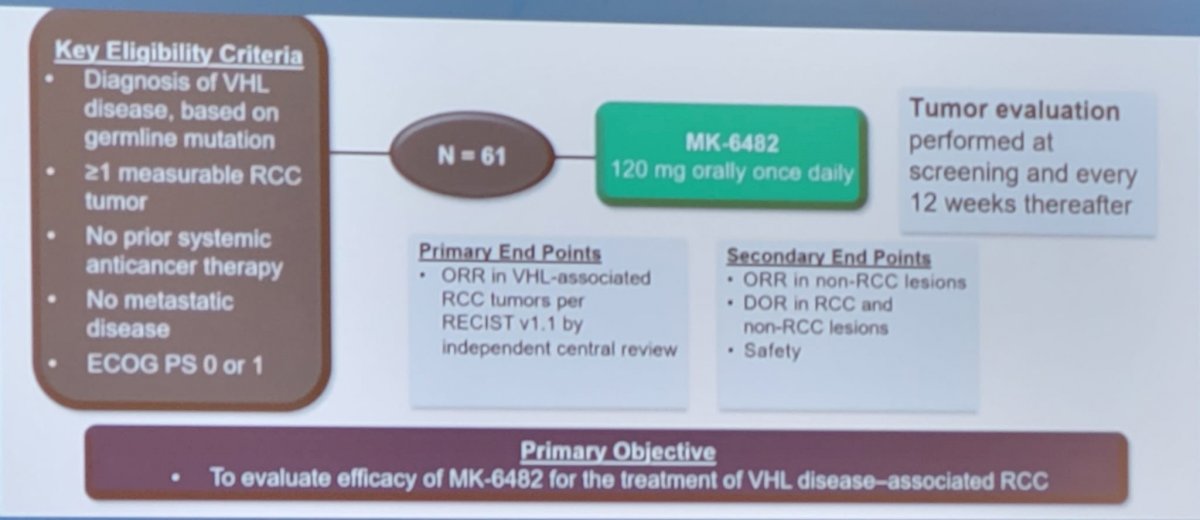
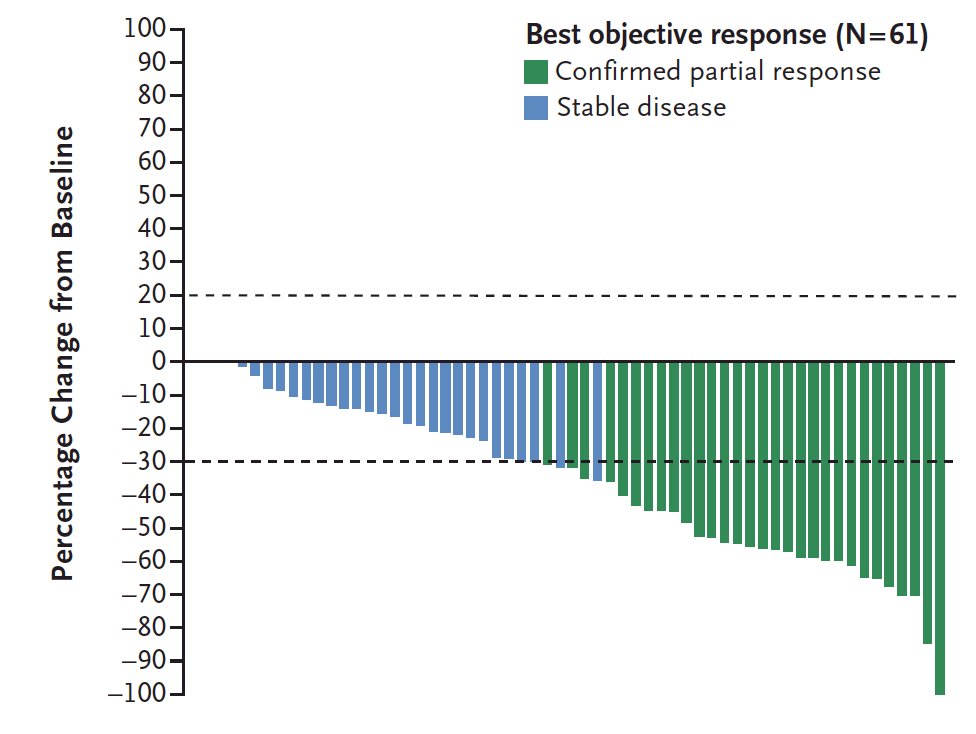
This phase 2 open-label trial investigated the efficacy and safety of the belzutifan administered orally at a dose of 120 mg daily, in patients with renal cell carcinoma associated with VHL disease. The primary endpoint was objective response (complete or partial response) and other assessments included responses to belzutifan in patients with non–renal cell carcinoma neoplasms and the safety of belzutifan. Over a median follow-up of 21.8 months (range, 20.2 to 30.1 months), the percentage of patients with RCC who had an objective response was 49% (95% CI, 36 to 62). There were no complete responses, but 49% of patients had partial response, 49% had stable disease, and only 3% of patients had progressive disease. Remarkably, a reduction in the sum of all target lesion diameters was observed in 56 patients (92%):
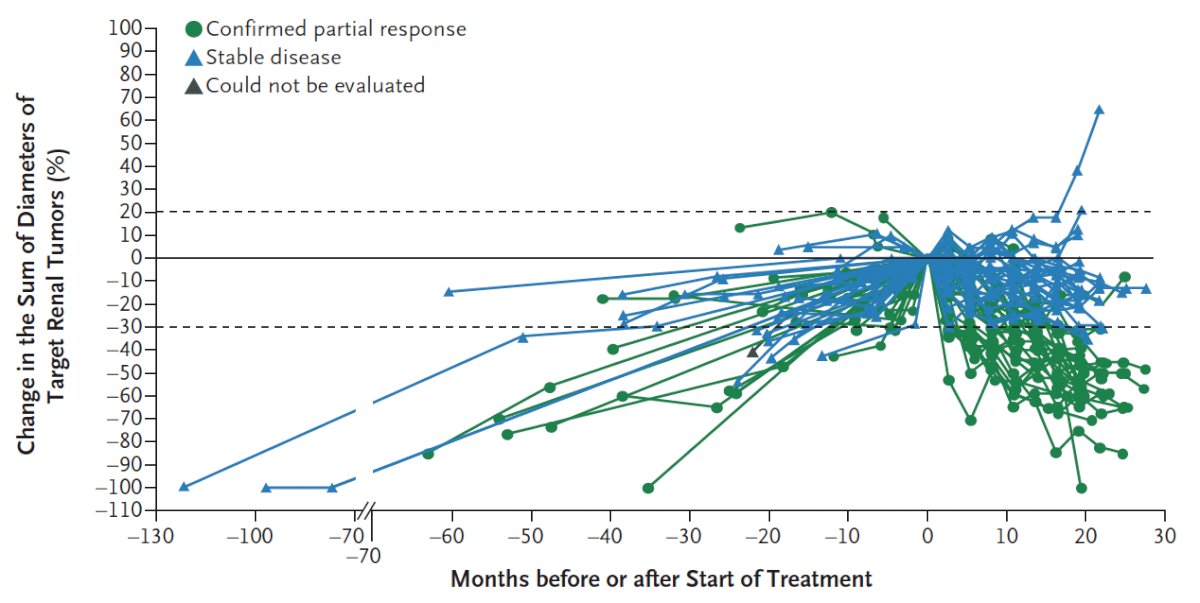
Most patients had growing tumors before treatment, followed by an observed reduction in the sum of the largest tumor diameters after treatment began:
The median time to response was 8.3 months, PFS at 24 months was 96%, 89% of patients were still on therapy at the time of data analysis, and median duration was not reached. The Swimmer’s plot for the duration of treatment is as follows:

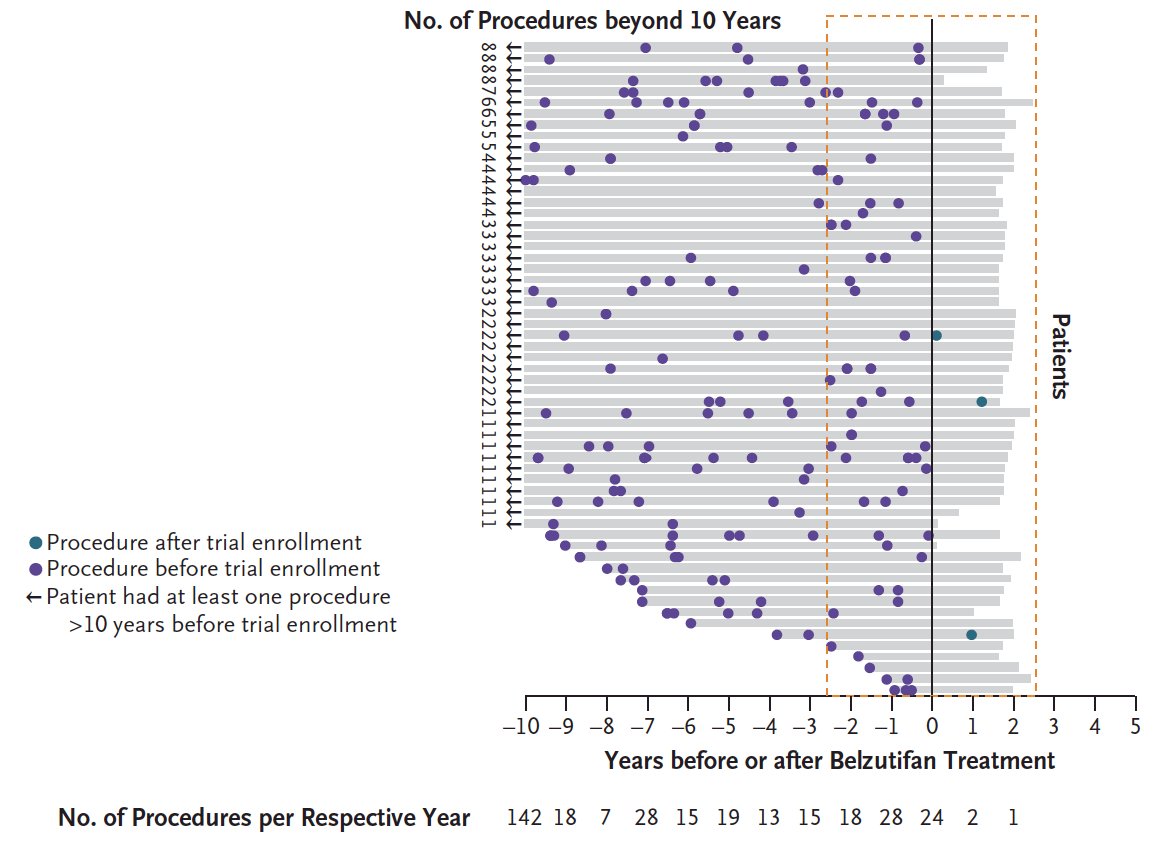
With regards to other sites of disease, responses were also observed in patients with pancreatic lesions (47 of 61 patients, 77%) and central nervous system hemangioblastomas (15 of 50 patients, 30%). Among the 16 eyes that could be evaluated in 12 patients with retinal hemangioblastomas at baseline, all were graded as showing improvement. Importantly, there were 327 procedures had been performed before treatment began, 64 of which had been
performed in the 2.5 years before treatment was started. There were very few procedures performed after starting belzutifan:
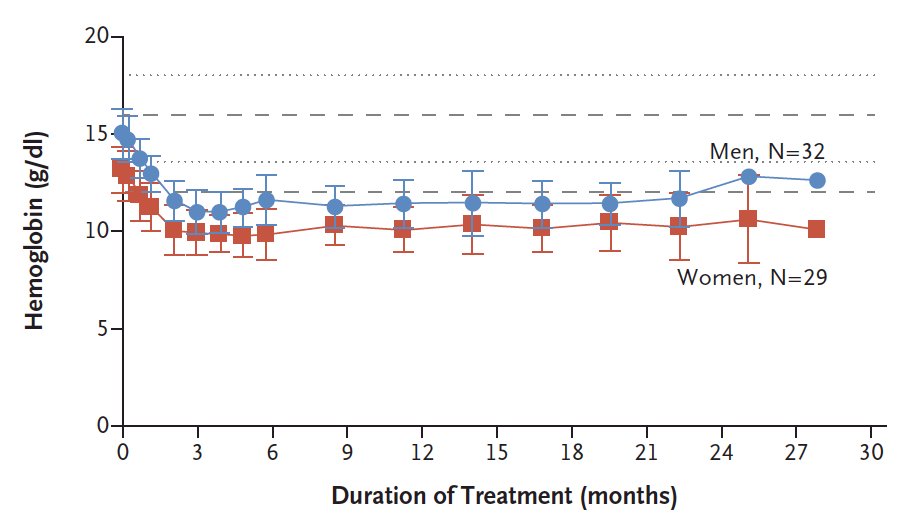
All patients had a decrease in hemoglobin levels from baseline of at least 1.9 g/dL
during the first 13 weeks of treatment, as was expected from on-target inhibition of the EPO gene, which reduces erythropoietin production:
There were 12 patients (20%) that received EPO stimulating agents with a median of 2.5 doses given. The most common adverse events were anemia (90% of patients) and fatigue (66% of patients). Seven patients discontinued treatment: four patients voluntarily discontinued, one discontinued owing to a treatment-related adverse event (grade 1 dizziness), one discontinued because of disease progression as assessed by the investigator, and one patient died (of acute toxic effects of fentanyl).
Based on the results of this trial, the FDA approved belzutifan for cancers associated with VHL disease on August 13, 2021. In the label, this is specific for patients that require therapy for associated RCC, central nervous system hemangioblastomas, or pancreatic neuroendocrine tumors not requiring immediate surgery.
Dr. Maranchie concluded her presentation by noting that there are several remaining questions/future studies:
- Timing of intervention
- Duration of response
- Mechanism of escape
- Duration of treatment: continuous versus intermediate, personalized dosing, etc
- Combination therapy
Presented by: Jodi K. Maranchie, MD, University of Pittsburgh Medical Center, Pittsburgh, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 Society of Urologic Oncology (SUO) Winter Annual Meeting, Orlando, FL, Wed, Dec 1 – Fri, Dec 3, 2021.
References:
- Maranchie JK, Vasselli JR, Riss J, et al. The contribution of VHL substrate binding and HIF1-alpha to the phenotype of VHL loss in renal cell carcinoma. Cancer Cell. 2002 Apr;1(3):247-255.
- Jonasch E, Donskov F, Iliopoulos O, et al. Belzutifan for Renal Cell Carcinoma in von Hippel-Lindau Disease. N Engl J Med. 2021;385:2036-2046.