There are well-known established prostate cancer risk factors, including age, family history, and race, which could stem from racism.
Systemic (institutional) racism is a form of racism that is embedded in the everyday operation of society. It produces and maintains systems/structures that operate via a process that disadvantages groups in a consistent manner across time and place. This ultimately produces disparities between groups that can be seen in:
- Wealth/employment
- Education
- Criminal justice/surveillance
- Housing
- Healthcare
Next, Dr. Mahal moved on to discuss the disparities in prostate cancer. Black men have a higher lifetime probability of developing and dying from prostate cancer (Table 1). Black men also have more advanced and aggressive disease at presentation (Figure 1).
Table 1 – Probability of being diagnosed and dying from prostate cancer: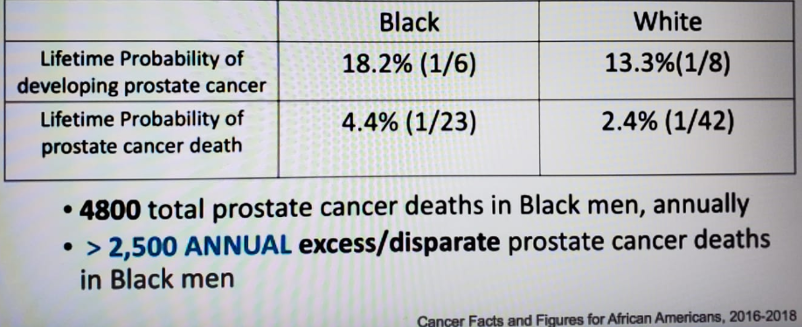
Figure 1 – Prostate cancer stratified by race: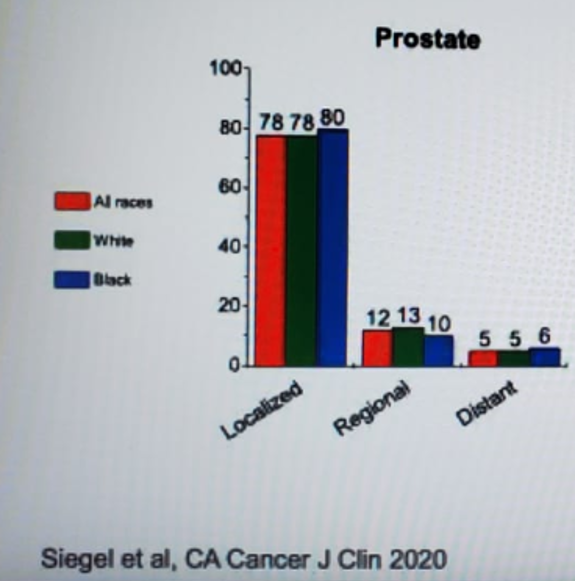
Despite having a greater prostate cancer burden and despite accounting for 12-14% of the United States (US) population, Black men are poorly represented in randomized clinical trials. For example, In the US PLCO screening trial, only 4.4% of men were Black. Additionally, 1/3 of the trials leading to drug approval from 2008-2013 did not report racial makeup, and in low-risk, conservative management trials, <1-2% of volunteers were Black. The only exceptions are several RTOG trials in localized prostate cancer that have enrolled approximately 20% Black men.
In the RTOG randomized controlled trial setting, the Black race was associated with a lower risk of prostate cancer-specific mortality in N0-1M0 prostate cancer (figure 2). Furthermore, in the mCRPC docetaxel trials, Black men had similar overall survival as White men (Figure 3).
Figure 2 – RTOG trial – prostate cancer-specific mortality and overall mortality stratified by race: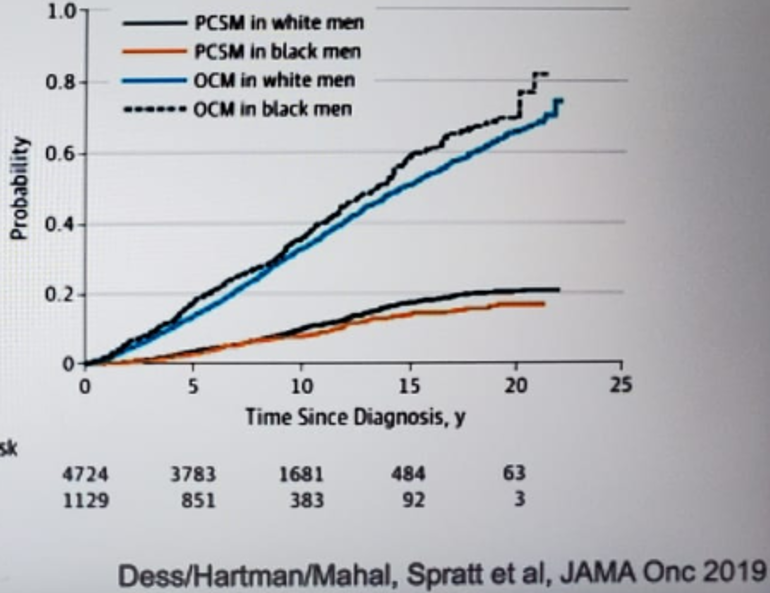
Figure 3 – Overall survival in White and Black men with prostate cancer: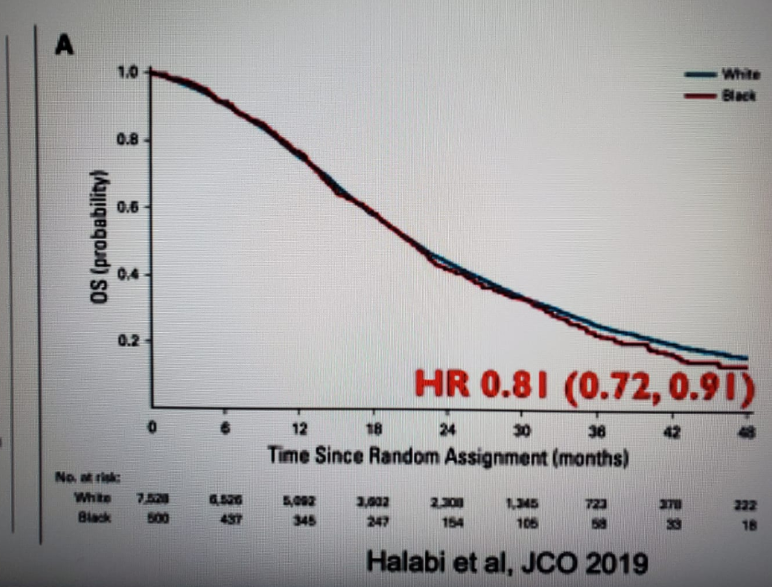
Equal access is the main goal we should attempt to reach. Unfortunately, there is data showing significant disparities in insurance rates among White and Black men (Table 2).
Table 2 – Insurance rates in Black and White men: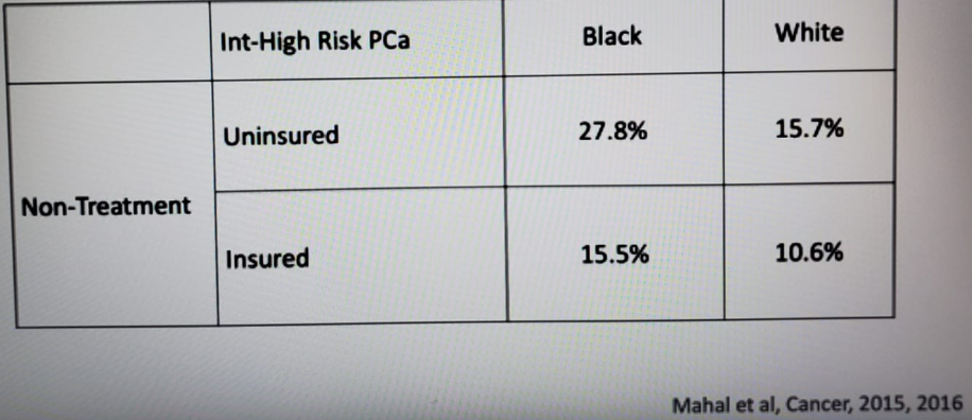
According to Dr. Mahal, the Affordable Care Act (ACA) eliminated racial disparities in coverage gaps. Before ACA (2000-2013), the Black race was associated with being uninsured (13.9% for Black vs. 10.4% for nonblack patients). After the ACA (2014-2017), there was no racial difference in the uninsured rate (6.9% for Black vs. 6.2% for nonblack patients)1.
Similar outcomes on survival curves in “equal” settings don’t entirely account for population mortality differences, as can be seen in Figure 4.
Figure 4 – Mortality difference in Black and White men:
Dr. Mahal moved on to discuss systemic racism and precision medicine/genomics in prostate cancer disparities. Trends in genomics and “precision medicine” may exacerbate disparities. Genomics risk scores are poised to improve risk-prediction and biomedical outcomes. However, most genomic studies are based on Eurocentric cohorts and therefore tend to be less accurate than others. Approximately 80% of all participants in the GWAS catalog are of European descent despite making only up to 16% of the population (Figure 5).
Figure 5 – Ancestry of GWAS participants over time as compared with the global population: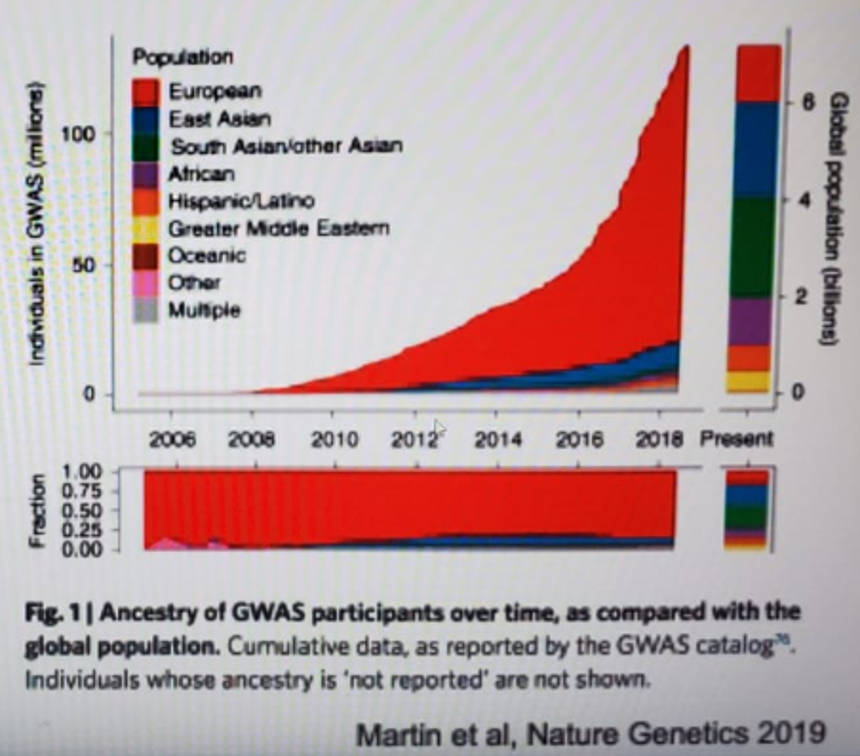
Integrated genomic alterations and ancestry analysis in TCGA show a higher frequency of TP53 mutations and SCNA/CCNE1 amplification and lower PI3K pathway alterations in African ancestry compared with European ancestry patients.
Structural racism is affected by many various factors (Figure 6), and racial disparities in prostate cancer are caused by a multitude of factors and interactions (Figure 7).
Figure 6 – Structural racism:
Figure 7 – Why are there racial disparities in prostate cancer: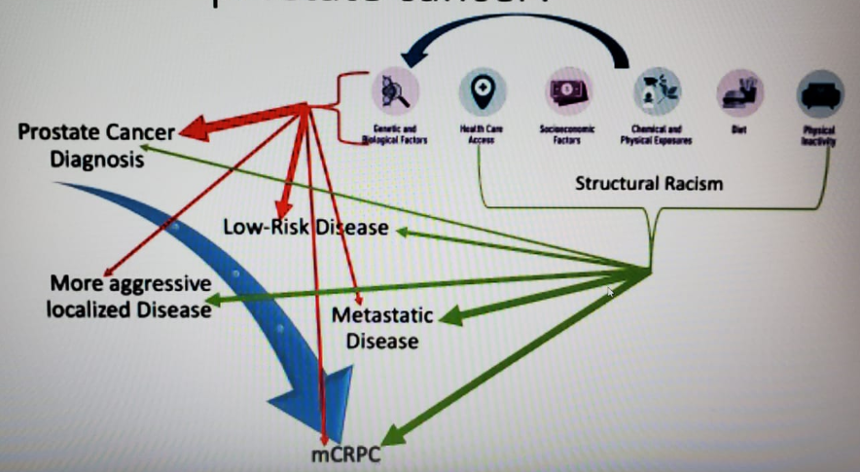
Currently, there are many unanswered questions. We need to better understand healthcare system factors, genetic susceptibility, social factors including racism, lifestyle factors, and health behaviors, tumor-related factors, and the interaction between genes and the environment (=The “biological” implications of racism).
In order to answer these many questions and address all prostate cancer disparities, several steps are required
- Creating a transdisciplinary approach for biologic, basic, clinical, and epidemiological research
- Clinical trials need to include a more diverse population
- Utilize “precision” medicine to identify mechanisms of disparity
- Outreach programs are needed to bring care delivery and cutting-edge science to diverse communities
- One of the biggest challenges is breaking the barrier of distrust that patients may feel towards the healthcare system altogether.
Dr. Mahal concluded his excellent talk by stating that involving patients and the community as partners rather than subjects is key. This needs to be done through community outreach and engagement, which works best with diverse oncology workforce, education, transparency, owning history of mistakes, acknowledging racism as a risk factor, and lastly, establishing close collaboration with minority community leaders and institutions.
Presentedby: Brandon Mahal, MD, University of Miami Miller School of Medicine, Sylvester, Comprehensive Cancer Center
Written by: Hanan Goldberg, MD, MSc, Assistant Professor, Urology Department, SUNY Upstate Medical University, Syracuse, NY, USA Twitter: @GoldbergHanan at the 2020 Society of Urologic Oncology Annual Meeting – December 2-5, 2020 – Washington, DC
References:
- Sanford NN, Lam MB, Butler SS, et al. Self-reported Reasons and Patterns of Noninsurance Among Cancer Survivors Before and After Implementation of the Affordable Care Act, 2000-2017. JAMA oncology 2019; 5(10): e191973.