At the 2020 Society of Urologic Oncology (SUO) virtual annual meeting, 3rd-year medical student Hriday Bhambhvani from Stanford University presented results of his group’s research assessing population-level associations of sociodemographic factors with chemotherapy, retroperitoneal lymph node dissection (RPLND), and survival among patients with non-seminomatous germ cell tumors (NSGCTs).
For this study, they used the Surveillance Epidemiology and End Results database (2005-2015) to identify 8,573 patients with NSGCTs. Multivariable logistic regression and Cox proportional hazards models were constructed to examine the association of sociodemographic factors (neighborhood socioeconomic status (nSES), race, insurance, and marital status) with, respectively, adjuvant chemotherapy/RPLND and overall survival.
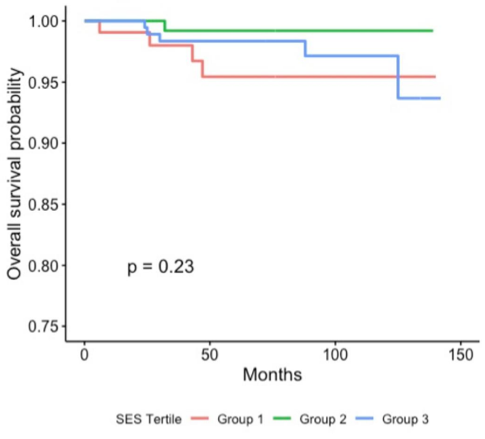
They found that low nSES (OR 0.59, 95% CI 0.40-0.88, p=0.01) and African American (OR 0.41, 95% CI, 0.15-1.00, p=0.058) patients with stage II disease were less likely to receive RPLND compared to high nSES and white patients, respectively. Stage III patients with Medicaid (OR 0.64, 95% CI 0.46-0.89, p=0.009) or those without insurance (OR 0.46, 95% CI 0.27-0.76, p=0.003) were less likely to receive RPLND compared to patients with private insurance. Furthermore, Asian (OR 0.62, 95% CI 0.45-0.86, p=0.005) and uninsured (OR 0.70, 95% CI 0.55- 0.88, p=0.003) patients with stage I disease were less likely to receive chemotherapy compared to white and privately insured patients, respectively. Finally, low nSES patients with stage I disease (HR 2.12, 95% CI 1.23-3.67, p=0.007) or stage II disease (HR 2.97, 95% CI 1.00-8.78, p=0.049) and African American patients with stage I disease (HR 1.97, 95% CI 1.01-3.85, p=0.046) had higher risks of all-cause mortality compared to high nSES and white patients, respectively. As follows are the Kaplan Meier curves for overall survival stratified by all Stage II patients:

Stage II patients that received post-chemotherapy RPLND:
All Stage III patients:

And stage III patients that received a post-chemotherapy RPLND:

Hriday Bhambhvani noted that it is important to have standardization of care, expansion of care, and improve diversity amongst providers with sustained recruitment of minorities. In conclusion, this population-level study found multilevel sociodemographic disparities in receipt of adjuvant therapy, including low nSES and African American patients with stage II disease being less likely to receiving post-chemotherapy RPLND. Additionally, there were stage-specific survival disparities among these patients with NSGCTs.
Presented by: Hriday Bhambhvani, Medical Student, Stanford University, Palo Alto, CA
Co-Authors: Daniel Greenberg, Alex Kasman, Mindy DeRouen, Iona Cheng, Michael Eisenberg, Sumit Shah
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md at the 2020 Society of Urologic Oncology Annual Meeting – December 2-5, 2020 – Washington, DC