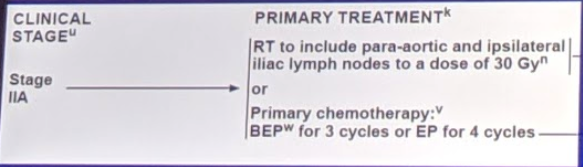
Current NCCN management of Stage IIA seminoma (low-volume metastatic disease) is:
RPLND has known efficacy in treating germ cell tumors – in the primary setting for NSGCT (stage 1 and 2) and in the post-chemotherapy setting for seminoma and NSGCT. Based on this, Dr. Daneshmand and Dr. Brian Hu (Loma Linda) hypothesized that it could be useful in low-volume seminoma patients as well.
In their pilot study of 4 patients, they found that patients did well – LOS was 3 days, one Clavien 1 complication, all maintained antegrade ejaculation, and no adjuvant therapy was required through 2 years. In updated follow-up, all four patients have not required additional therapy through 5 years.
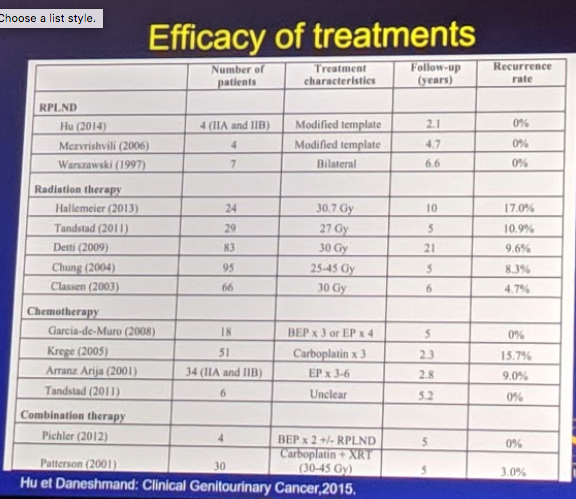
This in combination with other small series seemed to support the low recurrence rates following primary RPLND – much better than radiation or chemotherapy, as seen below:
This was the inception of the SEMS trials – with Drs. Daneshmand and Hu as co-primary investigators.
Inclusion criteria:
Pure seminoma
Stage 1 with 1-3 cm relapse OR presenting with stage IIA/B disease (no more than 2 lymph nodes, 1-3 cm in any direction)
LN must be in RPLND template
Imaging within 6 weeks of surgery
Normal serum tumor markers (1.5 ULN)
Relapse within 3 years of orchiectomy (to exclude late-relapse disease)
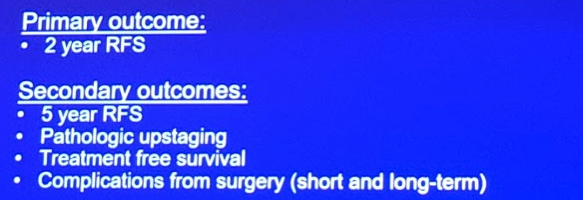
Outcomes planned are as follows:
Of note, similar to the SWOG studies, intra-operative photographs must be submitted to establish degree of node dissection.
Surgeon’s must meet volume requirements (8 RPLNDs/year or 24 in 3 years)
All are done open to remove one more variable
Planned accrual was for 55 patients over 4 years; 15 sites have been activated.
To date, 44 patients have been accrued.
Safety interim analysis has been met! Mostly Clavien 1-2 adverse events – 2 patients with Clavien 3: 1 PE and 1 chylous ascites.
The study is ongoing and they are almost done accruing patients. It will take 2 years for final results, but this may be a paradigm changing clinical trial! We look forward to the results.
Presented By: Siamak Daneshmand, MD
Written by: Thenappan Chandrasekar, MD, Clinical Instructor, Thomas Jefferson University, @tchandra_uromd, @TjuUrology, at the 19th Annual Meeting of the Society of Urologic Oncology (SUO), November 28-30, 2018 – Phoenix, Arizona