Another incentive to administer neoadjuvant chemotherapy over adjuvant chemotherapy, is the decline of renal function following radical nephroureterectomy. The Cisplatin eligibility rates decline from 58% before surgery to 15% post-surgery.
There are currently several ongoing trials of perioperative chemotherapy trials in upper tract disease patients as can be seen in figure 1.
Figure 1 – Ongoing and future trials of perioperative chemotherapy in UTUC patients:
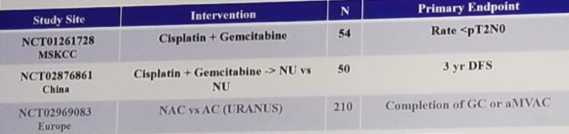
The URANUS trial (study design shown in figure 2) will be an important trial as it will assess and compare neoadjuvant to adjuvant chemotherapy to no chemotherapy at all for patients with T2-T4 N0-N1, M0 disease undergoing radical nephroureterectomy.
Figure 2 – URANUS trial design:

Concluding her talk, Dr. Hoffman-Censits compared between neaodjuvant and adjuvant chemotherapy. She began describing the most important points in the neoadjuvant setting stating that it might be over-treatment for some of the patients, it is treating micro-metastatic disease early on, and it is available for a greater number of patients (less renal impairment). It also harbors the opportunity to improve renal function and enables us to assess the sensitivity of the tumor to cisplatin. Lastly, it also leaves us the option to use adjuvant chemotherapy in non-responders.
She then moved on to discuss adjuvant chemotherapy. In contrast to neoadjuvant chemotherapy, there is no option for overtreatment, it does not treat micrometastatic disease at an early stage, due to renal impairment, it is not available for all patients, and it does not allow us to assess cisplatin sensitivity. Lastly, there is obviously no opportunity for adjuvant therapy in non-responders. Overall survival advantage is not clear for both adjuvant and neoadjuvant chemotherapy.
We will need to patiently await the results of the ongoing and recruiting prospective randomized trials to have more data.
Presented By: Jean Hoffman-Censits, Johns Hopkins Medicine
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow, SUO, University of Toronto, Princess Margaret Cancer Centre, @GoldbergHanan, at the 19th Annual Meeting of the Society of Urologic Oncology (SUO), November 28-30, 2018 – Phoenix, Arizona