Trimodal therapy (TMT) is a category 1 option for localized MIBC,4 which includes maximal transurethral resection of visible bladder tumor followed by radiotherapy in conjunction with radiosensitizing chemotherapy regimens.5 Generally accepted criteria for surgically fit patients suitable for this approach include those with small (<4-7cm) unifocal tumors, well-functioning bladders, and an absence of obvious extravesical extension, carcinoma in situ, or hydronephrosis.4 Although stringent, it is estimated that approximately one out of every five MIBC patients meet these criteria.6 In addition, there remains concerns regarding quality of TMT delivered in the real world setting which may impact oncologic outcomes.7
To date, randomized comparisons of TMT to RC are unavailable and are unlikely to be undertaken in the wake of SPARE, a phase III randomized control trial which launched in 2007 and prematurely closed due to poor accrual.8 Comparative outcomes are limited to observational studies with conflicting results. In a recent systematic review of 12 retrospective single center and population-based studies, overall survival outcomes varied significantly. Meta-analysis of the included single center studies showed a non-statistically significant advantage for TMT while the pooled estimate after adding the population-based studies favored RC.9 These results challenge large population-based studies which suggest TMT to be inferior to RC.7,10 These findings were recently challenged by abstract data presented at the 2022 American Society of Genitourinary Oncology meeting where a multicenter retrospective 3:1 matched comparison analysis of TMT (n=282) and RC (n=834) showed no difference in 5-year metastasis-free survival between treatments (78% vs. 73%, p=0.07) and a statistically significant cancer-specific and overall survival advantage in those treated with TMT (85% vs. 78%, p=0.02, 78% vs. 70%, p<0.001).11 Moreover, only 13% of patients undergoing TMT required salvage cystectomy for treatment failure or toxicity which has been often touted as another reason to avoid TMT. As retrospective and observational in nature and despite attention to control for known confounding these data cannot control for inherent bias, patient selection, and often lack long-term follow-up.
While patient selection and comorbidity of the TMT patients are included in retrospective analyses to date, there are several additional limitations important to consider when attempting to translate these data into clinical practice. First, a standard definition of TMT is lacking. Radiotherapy target volumes and fractionation vary in the literature and often do not correlate with prior level 1 evidence comparing TMT vs. radiotherapy alone.12 Similarly, while cisplatin-based regimens, gemcitabine monotherapy, or combination fluorouracil and mitomycin C are most common, there is lack of consensus on which radiosensitizing chemotherapy regimen to employ or how to employ it (i.e. split course vs. continuous course). The inclusion of neoadjuvant or adjuvant therapies to these treatments leads to even greater heterogeneity. Second, each of the three components of TMT requires multidisciplinary care to maximize outcomes. The quality of transurethral resection of bladder tumor (TURBT), radiation planning, surveillance, and chemotherapy management likely vary depending on the provider and introduce further unmeasured confounding. Finally, the criteria for continuing with TMT and management of progression vary between centers. For example, in an analysis of long-term outcomes in patients treated with TMT at Massachusetts General Hospital, a restaging post-induction TURBT was performed. Patients without a complete response were recommended to receive immediate RC (which was performed in 17% of all patients) instead of finishing the remaining consolidation treatment doses.13 Understanding the impact of such protocol variations on outcomes is critical.
Another option for understudies and underappreciated treatment option is radical TURBT with or without neoadjuvant chemotherapy. Indeed, among patients who underwent TURBT alone for MIBC, the 10-year disease-free survival was 76% with no difference in survival compared to those that underwent immediate RC.14 These results may be further improved with additional neoadjuvant chemotherapy. As previously reported, partial cystectomy among MIBC is limited as for TMT, with results having comparable outcomes among appropriate patients (inferior among all comers) but substantial costs even associated with partial cystectomy vs. RC.15
Lack of data describing long-term functional outcomes and treatment toxicity presents additional challenges to shared decision-making for bladder sparing options. Current literature would suggest that late severe toxicities such as end stage bladder and surgically managed bowel complications are rare (1-3%) and post-treatment quality of life is at least comparable to RC.16,17 However, the paucity of these data beyond 15 years, including the understudied possibility of secondary malignancy, makes evaluations of the appropriateness of TMT in younger populations with longer life expectancies challenging.
Finally, as we previously eluded, the impact of these treatment approaches on the healthcare system as well as patients’ finances must be considered. In an analysis of 2,963 patients included in the SEER-Medicare linked database, median total costs were significantly higher for TMT compared to RC resulting in a nationwide excess spending of $468 million.10 Substantial costs were associated with radiotherapy and pharmacy. Regarding the latter, RC had higher costs than TMT when neoadjuvant chemotherapy was used among RC patients thus highlighting further cost containment among cancer drugs. These findings do not take into account newer agents and immunotherapy options which are dramatically more costly than conventional treatments. 18 The extent to which patients are responsible for this added cost is unknown, but there is a clear need for further evaluation of potential financial toxicity in bladder cancer which is the most costly cancer.18,19
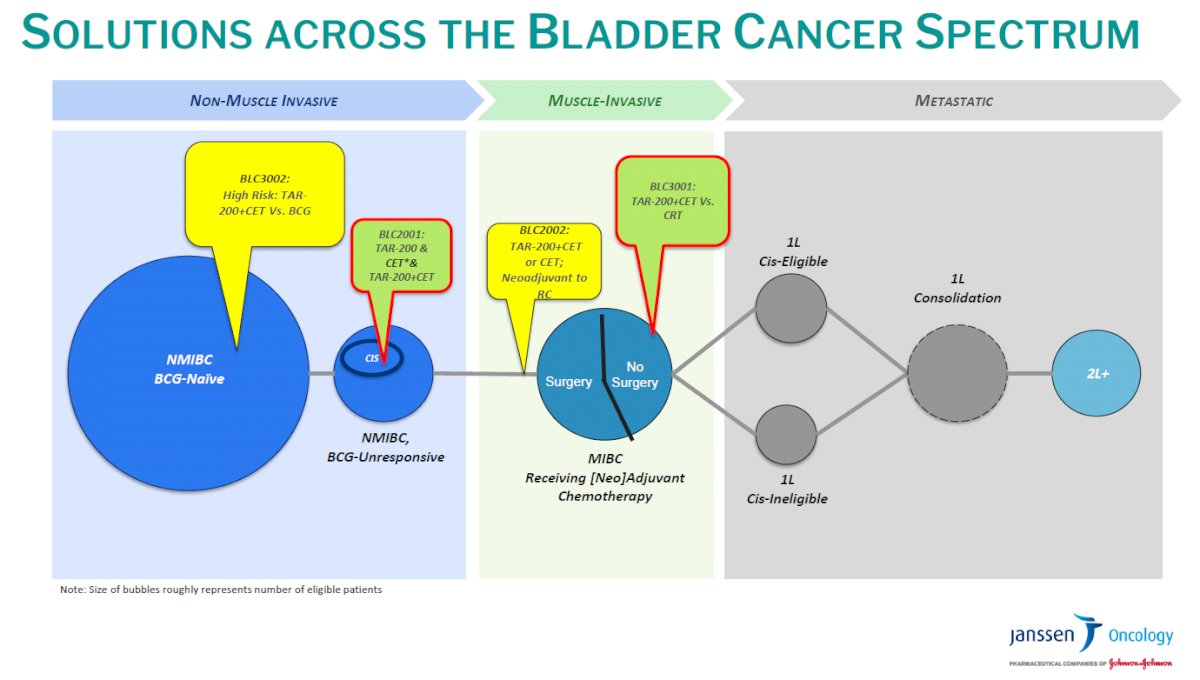
The utilization of TMT among other bladder sparing approaches is anticipated to grow as advancements occur. There are currently over half a dozen clinical trials evaluating the potential value of adding immune checkpoint inhibitors to TMT regimens. Biomarker directed therapy, application of novel intravesical drug delivery systems (such as TAR-200), advancements in disease imaging, and higher precision radiotherapy technology are just a few of the potential innovations that hold promise for continued improvement of oncologic outcomes and toxicity profiles associated with TMT. Indeed, TAR-200 offers acceptable toxicity but preliminary finding have shown up to 50% of patients that underwent TAR-200 insertion prior to RC had a partial or complete response.20 Current phase III trials are underway to investigate the use of TAR-200 in multiple disease states including a direct comparison to TMT among RC ineligible or refusing patients. SunRise-2 comparing TAR-200 + Cetrelimab vs. TMT has been open for enrollment since December 2022 with 274 sites worldwide and is expected to reach primary completion by December 2026 (NCT04658862).

This brings us to the critical topic in bladder cancer care which is leveraging the multidisciplinary approach to the patient. Oncologic, we need to embrace and engage all disciplines including medical oncology, radiation oncology, and urology. Importantly, urology should embrace bladder sparing options when appropriate but enroll patients in current bladder cancer trials. There are several excellent trials underway and near completion, but our patients need to be actively enrolled to understand this disease and improve outcomes fully. Additional, psycho-oncologic counseling with palliative care discussions have been underused in MIBC care and critical to optimizing survival outcomes. Prior studies have shown that 50% of MIBC patients that underwent definitive therapy with RC or TMT had a new onset psychiatric diagnosis which resulted in worse overall and cancer-specific survival. 21 Additionally, use of psychiatric drugs have been prescribed in 50% MIBC patients within 2 years of diagnosis with low adherence over time.22 Overall, 3972 (38%) patients had previous psychotropic prescriptions prior to cancer diagnosis, and these patients were much more likely to receive a post-cancer diagnosis prescription.22 Given the chronicity of psychiatric disorders with observed significantly low adherence to medications that warrants an emphasis on prolonged patient monitoring and further investigation.22 These findings further highlight the under-recognized and potentially lethal consequences of lack of mental health awareness in bladder cancer care. Moreover, palliative care use is dismal with on 3.6% of MIBC patients ever having a referral despite prior studies showing improved outcomes among those referred to palliative care early in their disease course.23 Taking the entire patient into account and engaging all services early on may further improve outcomes but also foster a shared commitment from all parties focused on the patient.
In summary, MIBC has expanded management options with the goal of bladder preservation taking center stage for providers and patients. The demographics, comorbidities, and preferences of MIBC patients along with promising oncologic outcomes are expanding use of bladder sparing options. However, the emergence of improved long-term evaluations of toxicity and quality of life in the context of oncologic outcomes and economic considerations are needed to understand which patients are most appropriate for bladder sparing approaches. Tomorrowland is no more and we live in an exciting time for bladder cancer care. We also live in a volatile health care climate with economic considerations on the forefront with value-based care providing the best care for every patient, every time more paramount than ever.
Presented by: Stephen B. Williams, MD, MS, FACS, Division of Urology, Department of Surgery, University of Texas Medical Branch, Galveston, TX
Written by: Stephen B. Williams, MD, MBA, MS @SWilliams_MD on Twitter during the South Central Section American Urological Association Annual Meeting, September 6-10, 2022, Coronado, CA
References:
- Williams SB, Huo J, Chamie K, et al. Underutilization of Radical Cystectomy Among Patients Diagnosed with Clinical Stage T2 Muscle-invasive Bladder Cancer. Eur Urol Focus. 2017;3(2-3):258-264.
- Gore JL, Litwin MS, Lai J, et al. Use of radical cystectomy for patients with invasive bladder cancer. J Natl Cancer Inst. 2010;102(11):802-811.
- Parekh DJ, Reis IM, Castle EP, et al. Robot-assisted radical cystectomy versus open radical cystectomy in patients with bladder cancer (RAZOR): an open-label, randomised, phase 3, non-inferiority trial. Lancet. 2018;391(10139):2525-2536.
- Flaig TW, Spiess PE, Abern M, et al. NCCN Guidelines® Insights: Bladder Cancer, Version 2.2022. J Natl Compr Canc Netw. 2022;20(8):866-878.
- Fletcher SA, Harmouch SS, Krimphove MJ, et al. Characterizing trends in treatment modalities for localized muscle-invasive bladder cancer in the pre-immunotherapy era. World J Urol. 2018;36(11):1767-1774.
- Smith ZL, Christodouleas JP, Keefe SM, Malkowicz SB, Guzzo TJ. Bladder preservation in the treatment of muscle-invasive bladder cancer (MIBC): a review of the literature and a practical approach to therapy. Bju Int. 2013;112(1):13-25.
- Williams SB, Shan Y, Jazzar U, et al. Comparing Survival Outcomes and Costs Associated With Radical Cystectomy and Trimodal Therapy for Older Adults With Muscle-Invasive Bladder Cancer. Jama Surg. 2018;153(10):881-889.
- Huddart RA, Hall E, Lewis R, Birtle A, Grp STM. Life and Death of Spare (Selective Bladder Preservation against Radical Excision): Reflections on Why the Spare Trial Closed. Bju Int. 2010;106(6):753-755.
- Wettstein MS, Rooprai JK, Pazhepurackel C, et al. Systematic review and meta-analysis on trimodal therapy versus radical cystectomy for muscle-invasive bladder cancer: Does the current quality of evidence justify definitive conclusions? Plos One. 2019;14(4).
- Williams SB, Shan Y, Ray-Zack MD, et al. Comparison of Costs of Radical Cystectomy vs Trimodal Therapy for Patients With Localized Muscle-Invasive Bladder Cancer. Jama Surg. 2019;154(8).
- Zlotta AR, Ballas LK, Niemierko A, et al. Multi-institutional matched comparison of radical cystectomy to trimodality therapy for muscle-invasive bladder cancer. J Clin Oncol. 2022;40(6).
- James ND, Hussain SA, Hall E, et al. Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med. 2012;366(16):1477-1488.
- Efstathiou JA, Spiegel DY, Shipley WU, et al. Long-term outcomes of selective bladder preservation by combined-modality therapy for invasive bladder cancer: the MGH experience. Eur Urol. 2012;61(4):705-711.
- Herr HW. Transurethral resection of muscle-invasive bladder cancer: 10-year outcome. J Clin Oncol. 2001;19(1):89-93.
- Bagheri I, Shan Y, Klaassen Z, et al. Comparing Costs of Radical Versus Partial Cystectomy for Patients Diagnosed With Localized Muscle-Invasive Bladder Cancer: Understanding the Value of Surgical Care. Urology. 2021;147:127-134.
- Rodel C, Grabenbauer GG, Kuhn R, et al. Combined-modality treatment and selective organ preservation in invasive bladder cancer: Long-term results. J Clin Oncol. 2002;20(14):3061-3071.
- Mak KS, Smith A, Eidelman A, et al. Quality of life in long-term survivors of muscle-invasive bladder cancer. J Clin Oncol. 2015;33(7).
- Khaki AR, Shan Y, Nelson RE, et al. Cost-effectiveness analysis of neoadjuvant immune checkpoint inhibition vs. cisplatin-based chemotherapy in muscle invasive bladder cancer. Urol Oncol. 2021;39(10):732.e739-732.e716.
- Dee EC, Chino F. Financial Hardship in Cancer Care-The Need to Define and Intervene on Actionable Metrics. JAMA Netw Open. 2022;5(7):e2223149.
- Daneshmand S, Brummelhuis ISG, Pohar KS, et al. The safety, tolerability, and efficacy of a neoadjuvant gemcitabine intravesical drug delivery system (TAR-200) in muscle-invasive bladder cancer patients: a phase I trial. Urol Oncol. 2022;40(7):344.e341-344.e349.
- Jazzar U, Yong S, Klaassen Z, et al. Impact of psychiatric illness on decreased survival in elderly patients with bladder cancer in the United States. Cancer. 2018;124(15):3127-3135.
- Jazzar U, Bergerot CD, Shan Y, et al. Use of psychotropic drugs among older patients with bladder cancer in the United States. Psychooncology. 2021;30(6):832-843.
- Hugar LA, Lopa SH, Yabes JG, et al. Palliative care use amongst patients with bladder cancer. Bju Int. 2019;123(6):968-975.