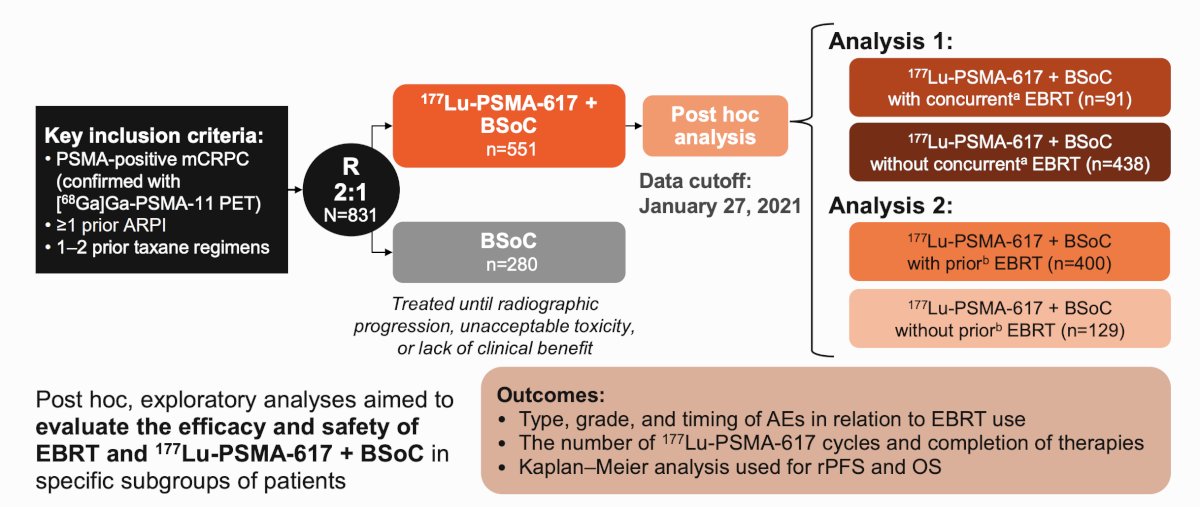
(UroToday.com) The 2026 SNMMI annual meeting featured a genitourinary radiotherapeutics session and a presentation by Dr. Abigail Pepin discussing a secondary analysis of the VISION trial assessing the impact of external beam radiotherapy use and timing on clinical outcomes in patients receiving 177Lu-PSMA-617 + best standard of care. In the phase III VISION (NCT03511664) study1, addition of the PSMA-targeted radioligand therapy 177Lu-PSMA-617 to the best standard of care resulted in statistically significant and clinically meaningful improvements in overall survival and radiographic progression-free survival in patients with progressive metastatic castration-resistant prostate cancer (mCRPC). In this post hoc secondary analysis, Dr. Pepin and colleagues evaluated the safety and efficacy of external beam radiotherapy and 177Lu-PSMA-617 + best standard of care.
This was a secondary analysis of the prospective randomized phase III VISION clinical trial that included patients diagnosed with mCRPC who had received ≥1 prior androgen receptor pathway inhibitor (ARPI) and 1–2 taxane-based chemotherapy regimens. In this analysis, patients from VISION who received 177Lu-PSMA-617 + best standard of care were included and then analyzed in two groups according to timing (Analysis 1) and use (Analysis 2) of external beam radiotherapy. Analysis 1 further categorized patients into those who received prior external beam radiotherapy versus no prior external beam radiotherapy before 177Lu-PSMA-617 therapy. Analysis 2 included patients who received concurrent vs no concurrent external beam radiotherapy during 177Lu-PSMA-617 therapy. Concurrent external beam radiotherapy was defined as external beam radiotherapy given on or after the start of 177Lu-PSMA-617 or was ongoing at the start of 177Lu-PSMA-617 but no more than 30 days after the end of 177Lu-PSMA-617 or the best standard of care (whichever was last). The overall response rate was defined as the proportion of patients whose best overall response was either a complete response or partial response, and the disease control rate defined as the proportion of patients with a best overall response of complete response, partial response or stable disease as per RECIST 1.1 criteria. Type, grade, and timing of adverse events in relation to external beam radiotherapy use (either prior [defined as adverse events occurring within 28 days prior to external beam radiotherapy] or after [defined as adverse events occurring within 28 days after external beam radiotherapy]) were assessed. Treatment patterns, including number of 177Lu-PSMA-617 cycles and completion of therapies, were also evaluated:
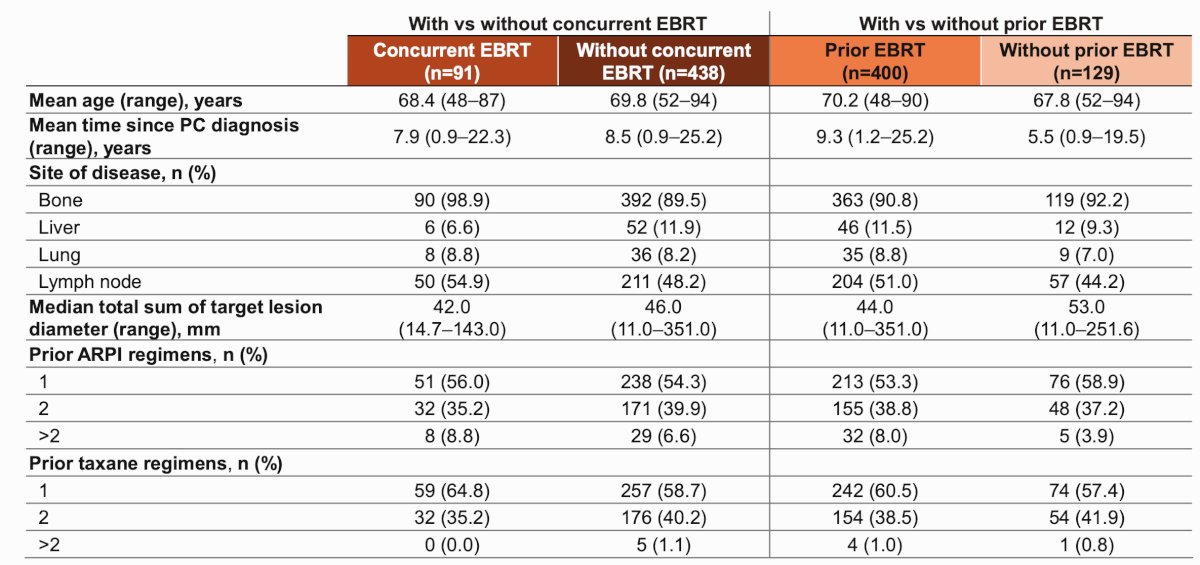
Data were analyzed descriptively, with Kaplan–Meier analysis used for time-to-event data. Across the post-hoc subgroups, the following baseline characteristics were similar:
In Analysis 1 (n = 529), patients with prior external beam radiotherapy (n = 400) had the same median number of 177Lu-PSMA-617 cycles (5 cycles) to patients without prior external beam radiotherapy (n = 129). In Analysis 2 (n = 529), patients with concurrent (n = 91) and without concurrent external beam radiotherapy (n = 438) had the same median number of 177Lu-PSMA-617 cycles (5 cycles):
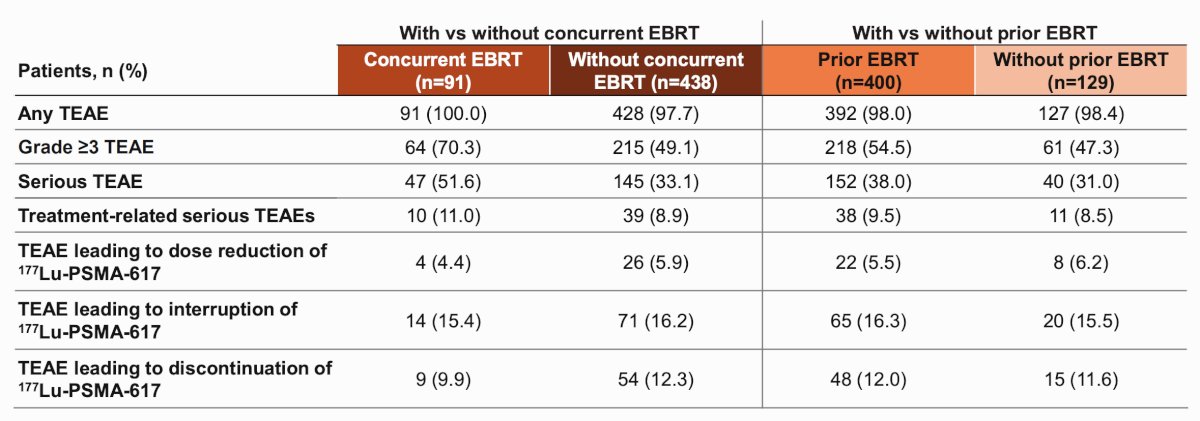
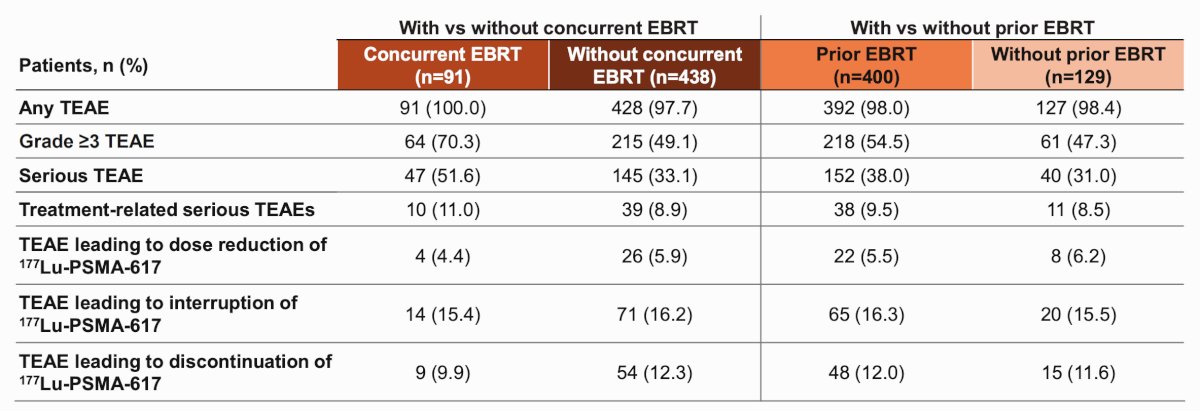
Adverse events were experienced in both sets of analyses; however, adverse events which led to the reduction, interruption, and discontinuation of 177Lu-PSMA-617 were numerically lower in the concurrent external beam radiotherapy group when compared to patients without concurrent external beam radiotherapy (4.4% versus 5.9%; 15.4% versus 16.2% and 9.9% versus 12.3%, respectively). Serious adverse events occurred in 51.6% of patients with concurrent external beam radiotherapy and in 33.1% without concurrent external beam radiotherapy; however, with respect to the timing of serious adverse events, 20.9% occurred prior to external beam radiotherapy and 14.3% occurred after external beam radiotherapy in patients receiving 177Lu-PSMA-617 + best standard of care with concurrent external beam radiotherapy:
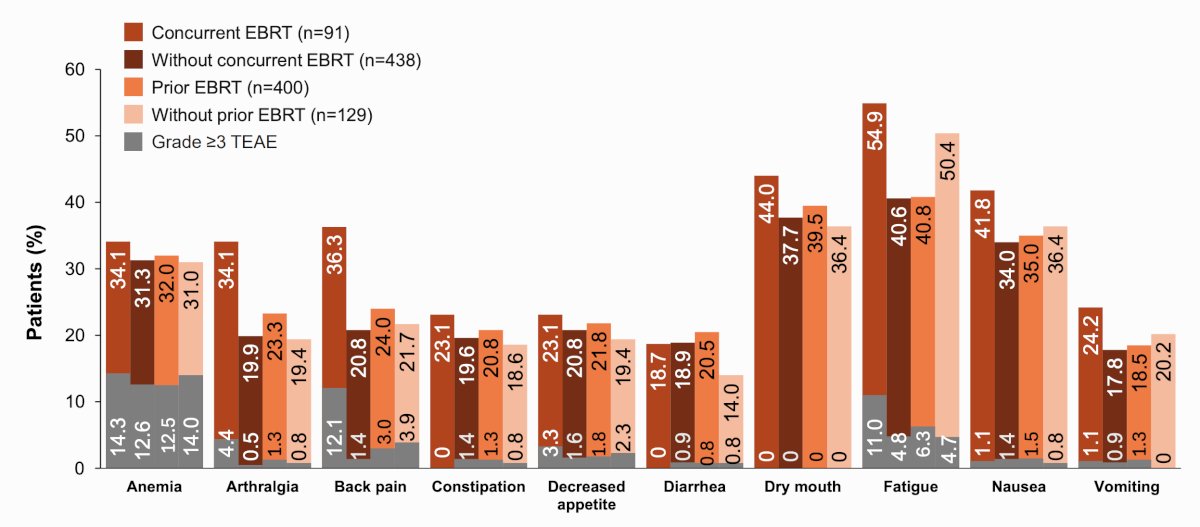
Treatment emergent adverse events reported in >= 20% of patients in any subgroup are highlighted in the following figure, most commonly anemia, dry mouth, fatigue, and nausea:
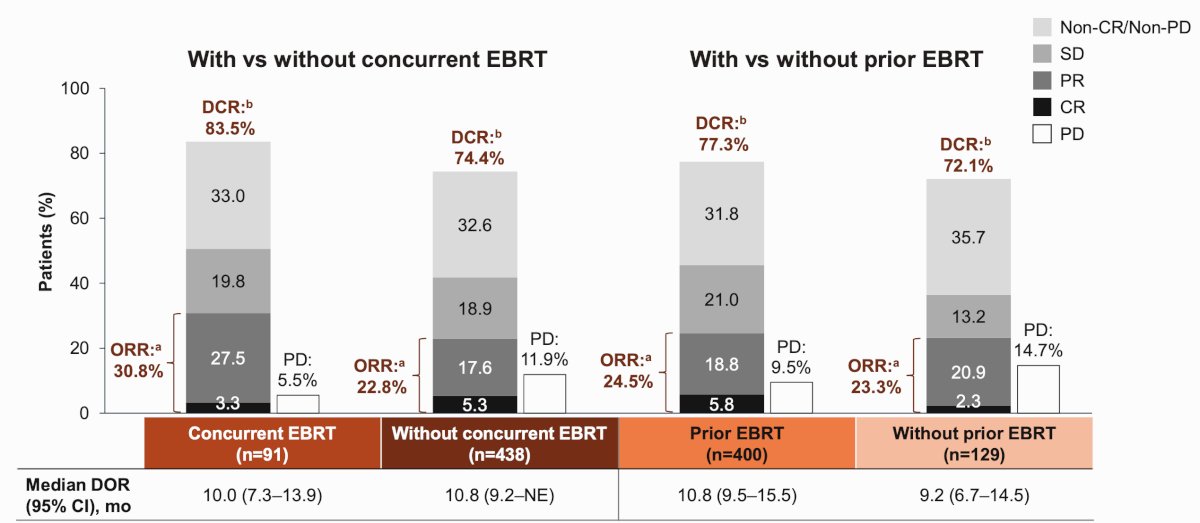
In patients with RECIST evaluable disease at baseline, the overall response rate was 24.5% in patients with prior external beam radiotherapy (n=98) compared with 23.3% for those with no prior external beam radiotherapy (n = 30). Disease control rate in these groups were 77.3% and 72.1%, respectively. The overall response rate and disease control rate in patients with concurrent versus without concurrent external beam radiotherapy was 30.8% versus 22.8% and 83.5% versus 74.4%, respectively:
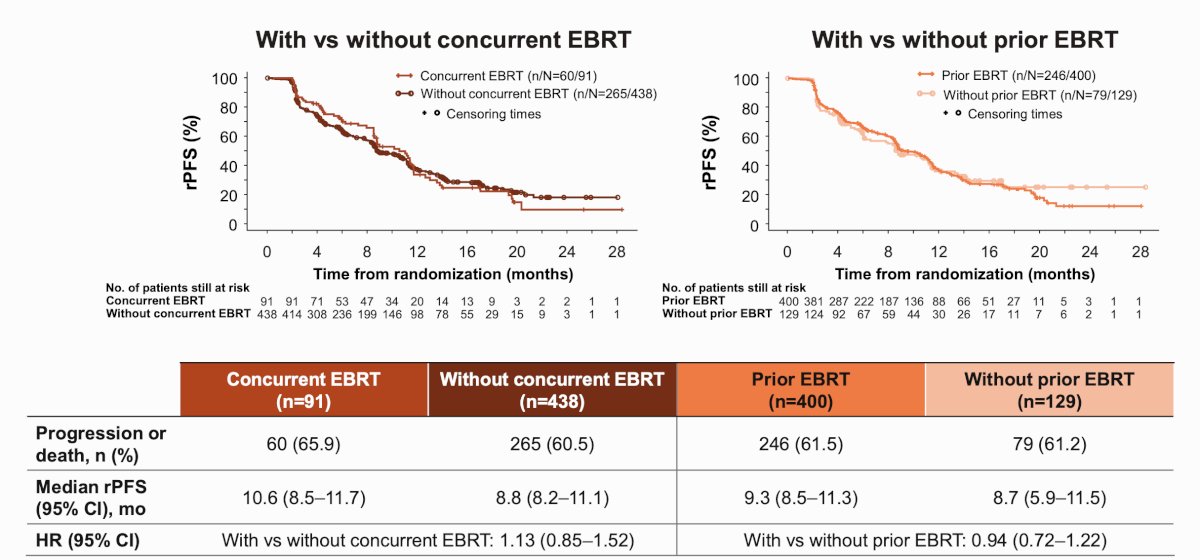
Radiographic progression-free survival was similar in patients with or without external beam radiotherapy in both analyses:
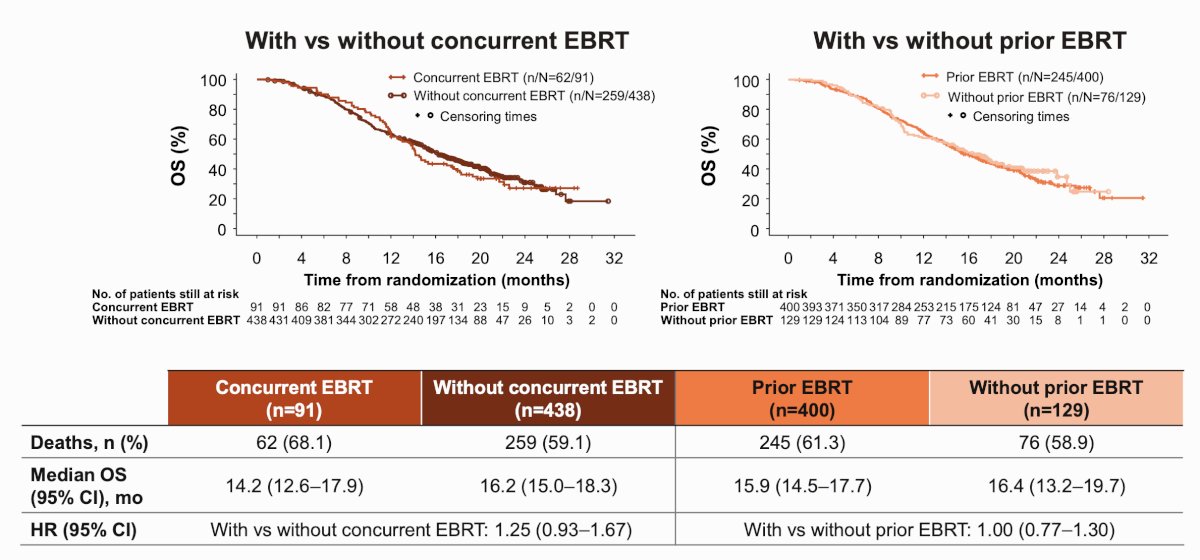
Overall survival was also similar in patients with or without external beam radiotherapy in both analyses:
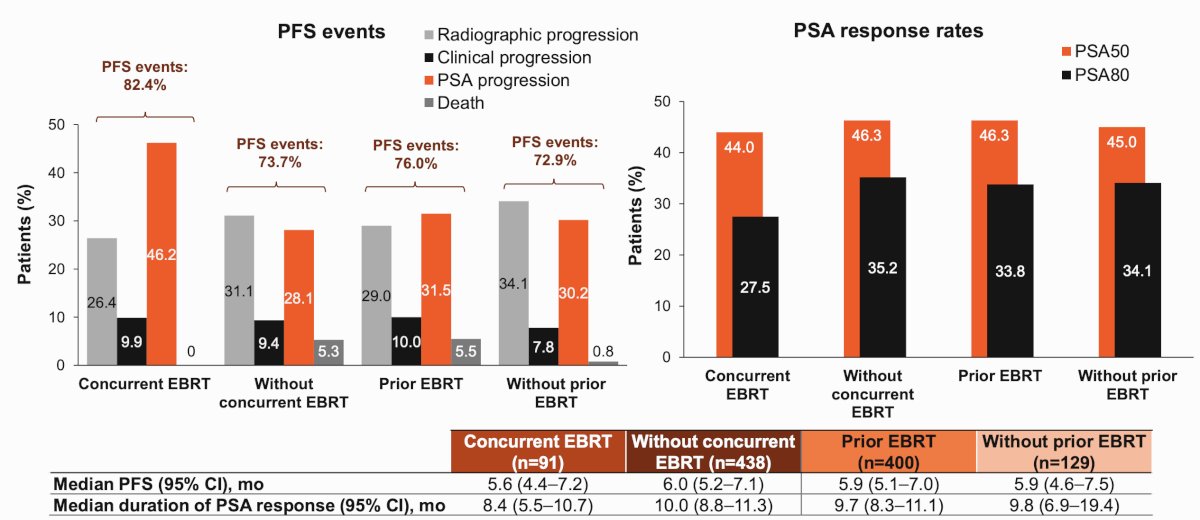
Across all subgroups, patients had similar progression-free survival and PSA response rates:
Dr. Pepin concluded her presentation discussing a secondary analysis of the VISION trial assessing the impact of external beam radiotherapy use and timing on clinical outcomes in patients receiving 177Lu-PSMA-617 + best standard of care, with the following take-home points:
- The median number of 177Lu-PSMA-617 cycles was similar between subgroups in both analyses, highlighting that external beam radiotherapy did not negatively impact treatment duration or completion
- Despite a higher incidence of serious treatment-emergent adverse events in patients with versus without concurrent external beam radiotherapy, patients were able to complete therapy with 177Lu-PSMA-617 + best standard of care at the same rates, irrespective of whether external beam radiotherapy was received
- Higher incidence of serious treatment-emergent adverse events, specifically back pain and spinal cord compression, in the concurrent external beam radiotherapy group ≤28 days before external beam radiotherapy, suggests these events likely led to the initiation of external beam radiotherapy
- Patients receiving concurrent external beam radiotherapy had comparable but numerically lower rates of treatment interruption and discontinuation, and numerically higher objective response rate and disease control rate, versus patients without concurrent external beam radiotherapy
- In both subgroup analyses, no notable differences in overall survival or progression-free survival were observed between external beam radiotherapy subgroups, demonstrating that external beam radiotherapy had no detrimental effect on outcomes in patients treated with 177Lu-PSMA-617 + best standard of care; however, these results should be interpreted with caution given the post hoc, exploratory nature of the analysis
Presented by: Abigail Pepin, MD, University of Pennsylvania Abramson Cancer Center, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Society of Nuclear Medicine and Molecular Imaging (SNMMI) 2026 Annual Meeting, Los Angeles, CA, Sat, May 30 – Tues, Jun 2, 2026.
References: