(UroToday.com) The 2025 SNMMI annual meeting featured a prostate cancer session and a presentation by Dr. Sabina Dizdarevic discussing sequencing and combining beta and alpha targeted radionuclide treatments in the management of patients with prostate cancer. Dr. Dizdarevic started her presentation by highlighting two main principles of nuclear medicine radiotheranostics in prostate cancer:
- Mechanism mediated targeted bone treatment – there is a similar mechanism of action with different elements/isotopes and different energy, whether this is 99mTc diphosphonates (gamma) or 18F-NaF positron/radium-223 (alpha) or 99Str (beta)
- Radioligand therapy: the same ligand/peptide, but different label/radioisotope. Ie. PSMA compounds but different labels with either beta (68Ga/18F) or gamma (99mTc) emitting radioisotopes for imaging, and subsequently beta (177Lu) or alpha (225Ac) emitting radionuclides for treatment
With regards to radium-223, the following provides proof of principle for targeted alpha therapies:
- Delivery of high, localized energy that is lethal to cancer cells, but minimizes damage to nearby tissues
- Radium-223 is the first FDA and EMA approved targeted alpha therapy
- Radium-223 has demonstrated “proof of concept” for this therapeutic approach
Radium-223 occurs naturally, but for medical use, man-made material is used; thus, radium-223 is a by-product material. Actinium-227 decays to radium-223 through thorium-227 (half life 1.77 years), and the actinium-227 source was produced by neutron irradiation of radium-226 in a reactor:

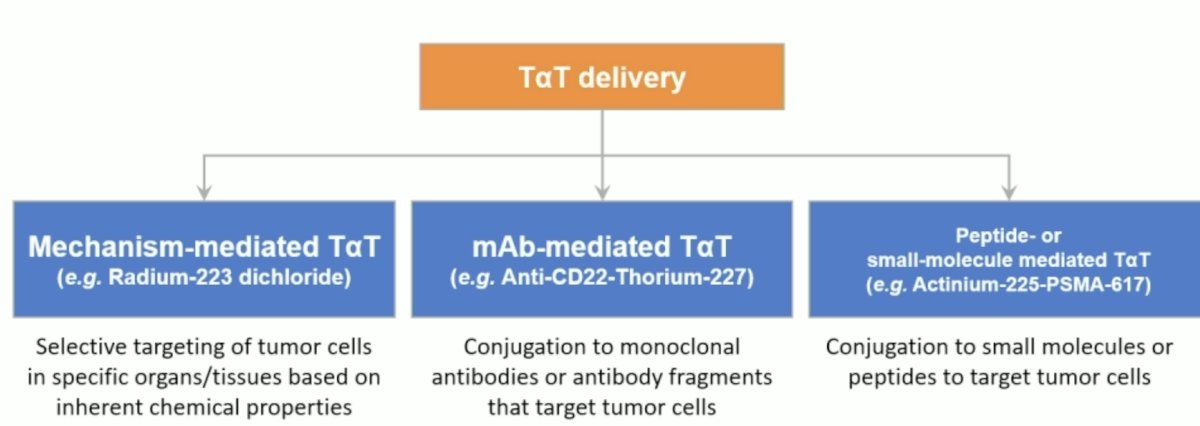
Moreover, radium-223 is incorporated into areas of high bone turnover in bone metastases, where it is shown to inhibit cancer cell proliferation and stabilize the bone microenvironment. Radium-223 has demonstrated a significant improvement in overall survival and patient quality of life exhibited a favorable safety profile. Dr. Dizdarevic provided the following categorization of targeted alpha therapies by method of delivery:
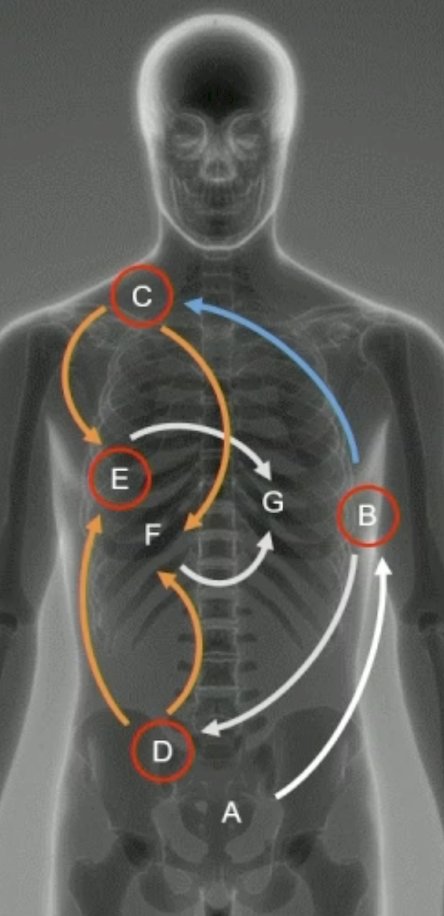
Additionally, bone can also be the source of other metastases. Once prostate cancer cells metastasize beyond the initial tumor site, they normally spread to an initial metastatic site in the bone. Tumor cells circulate in the blood and go from an initial metastatic site to subsequent metastatic sites within the bone. Metastases usually spread between distant sites rather than as separate waves from the primary tumor. Metastatic spread to other tissues outside the bone occurs in later stages of the disease, and metastasis outside the bone frequently involves spread to the liver:
Clinically, radium-223 emerged as a benefit for bone metastatic mCRPC based on the ALSYMPCA trial, published in 2013.1 Since ALSYMPCA, a large body of real world evidence for radium-223 has been published, and the treatment landscape has continued to evolve. Specifically, >100,000 patients with mCRPC have been treated with radium-223 in clinical practice since 2022.
The evolving treatment landscape in prostate cancer has resulted in a call to shift from protocol driven to biology driven care. But, Dr. Dizdarevic asks: Can we see what we treat?
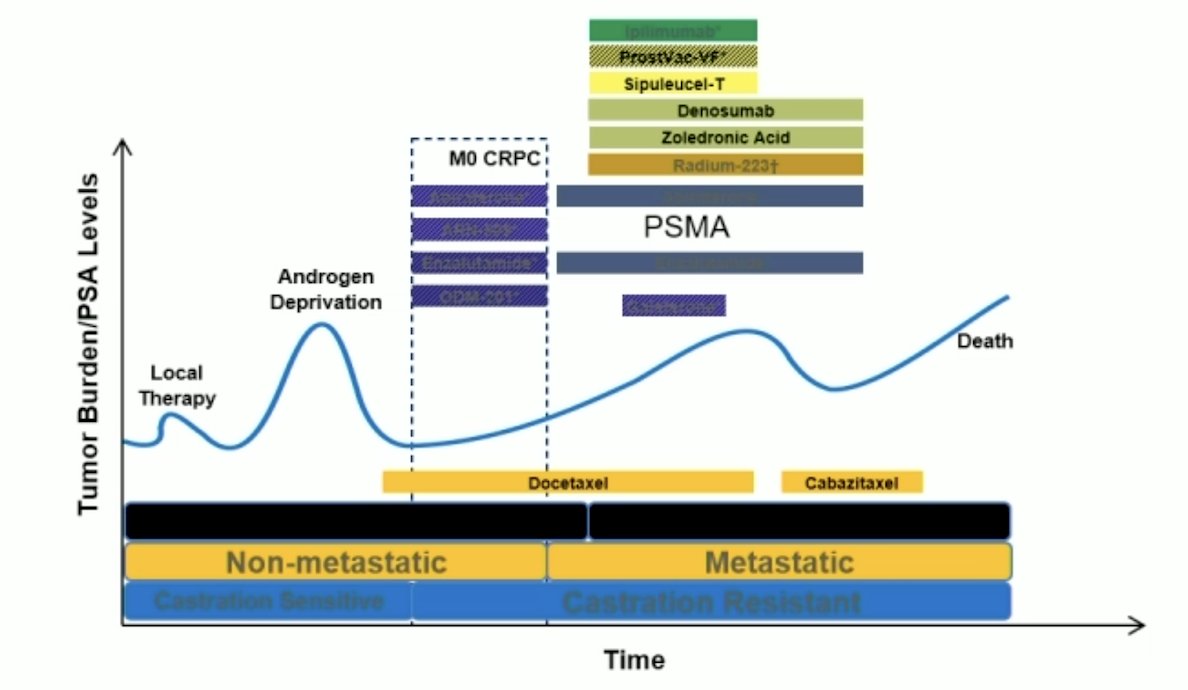
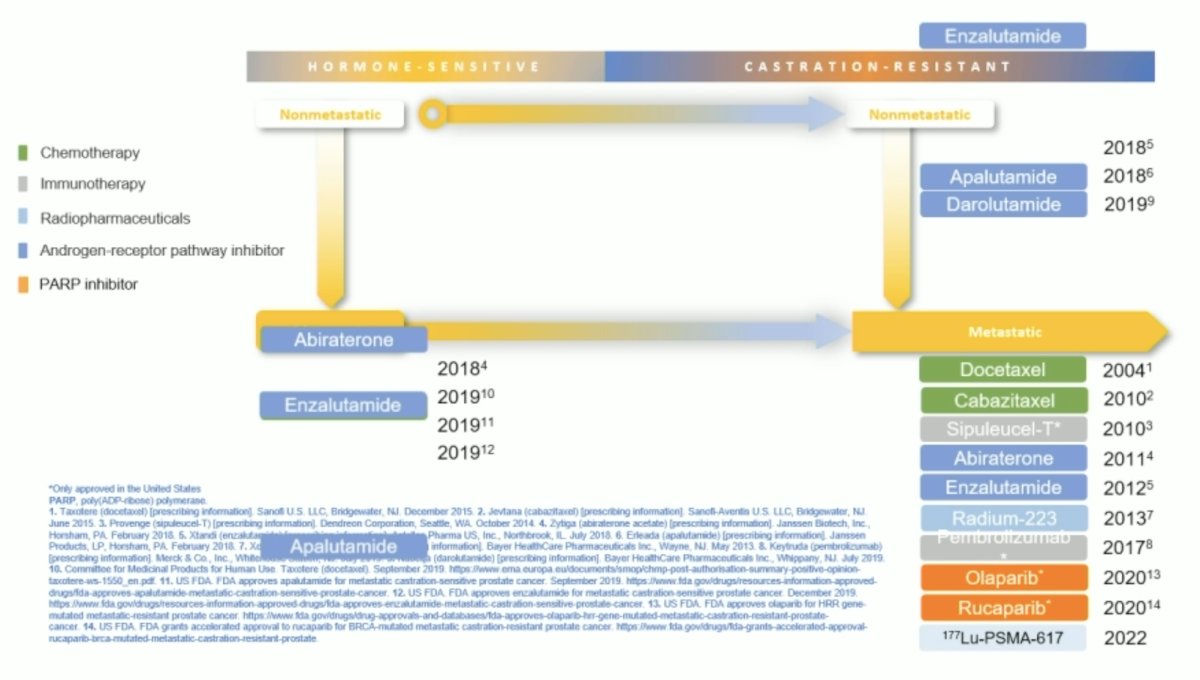
Notably, the approval of therapies in earlier stages of prostate cancer provides new opportunities for sequencing therapies to benefit patients:
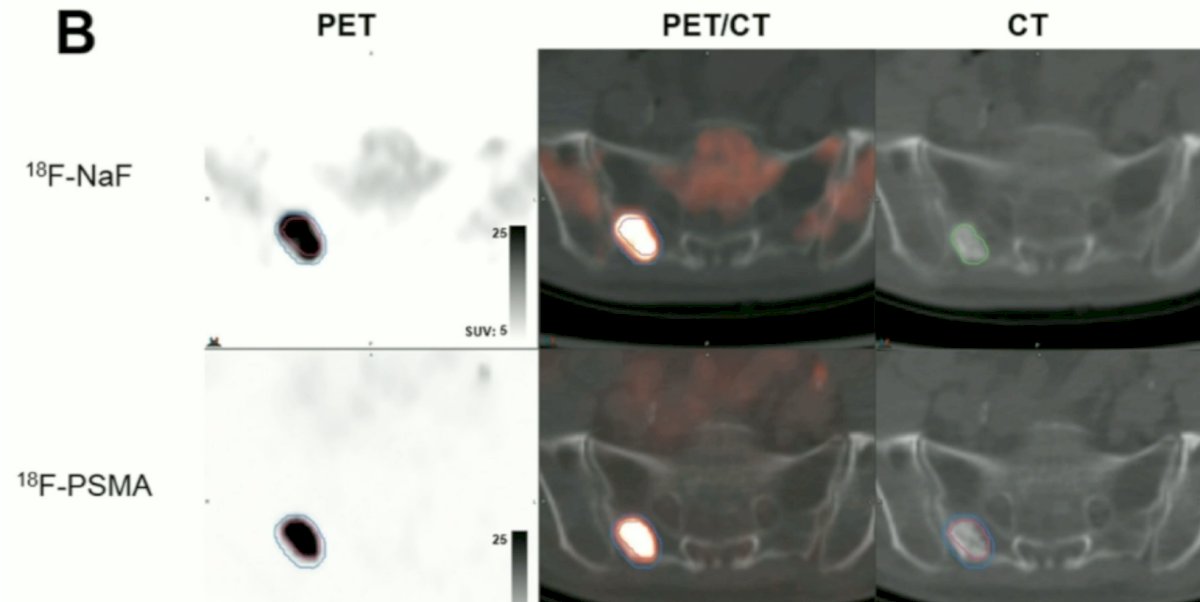
Dr. Dizdarevic emphasized that there is added value of 68Ga-PSMA PET/CT for the detection of bone metastases in patients with newly diagnosed prostate cancer and a previous 99mTc bone scintigraphy. However, 10% of these patients have a negative PSMA PET/CT. With regards to NaF and PSMA PET uptake, as metastatic prostate cancer progresses from castration-sensitive to castration-resistant disease, greater discordance is observed between NaF PET and PSMA PET uptake. This may indicate a possible phenotypic shift to tumor growth that is more independent of bone remodeling via osteoblastic formation.
Dr. Dizdarevic then discussed a comparison of prostate cancer bone metastases on 18F-sodium fluoride and 18F-PSMA PET/CT and discordance of uptake in the same lesion.2 The following two examples highlight this discordance:
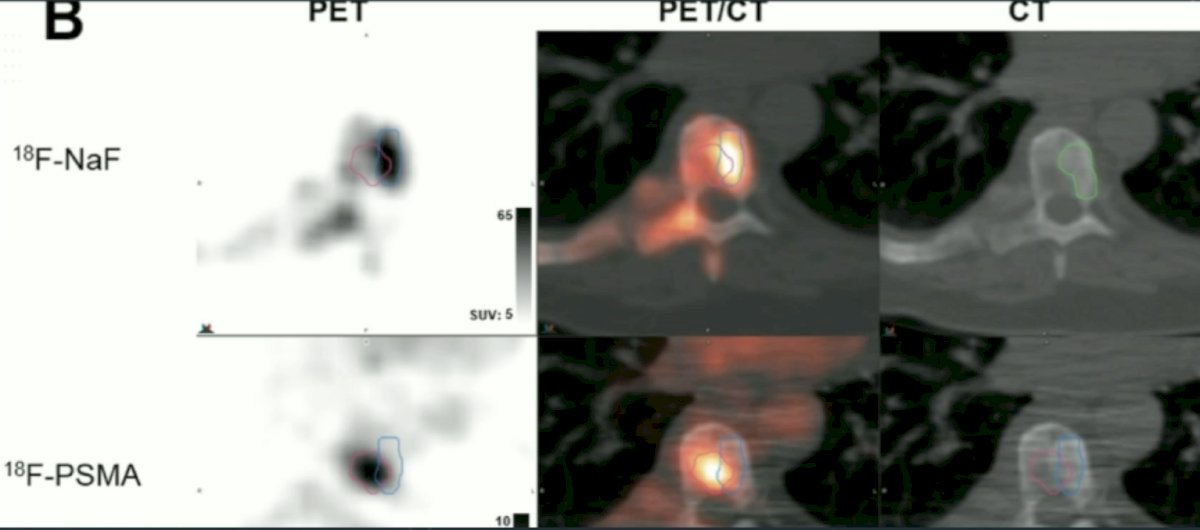
A comparison of 68Ga-PSMA-11 PET/CT with 18F-NaF- PET/CT in the evaluation of bone metastases in metastatic prostate cancer patients showed that 18F-NaF- PET/CT detects a higher number of pathologic bone lesions and high intensity (T/B 9.8 versus 5.9) in advanced stage prostate cancer patients scheduled for radionuclide therapy than 68Ga-PSMA-11 PET/CT. Thus, perhaps combined multi-tracer imaging is needed for patient selection prior to targeted radionuclide treatments.
What about radium-223 following 177Lu-PSMA radioligand therapy? In the VISION trial,4 2.5% of patients received radium-223 following 177Lu-PSMA radioligand therapy, and 17.4% of all patients had prior radium-223 treatment. Subsequently, the Advanced Prostate Cancer Consensus Conference (APCCC) emphasized that using 177Lu-PSMA radioligand therapy after radium-223 is safe (76% consensus), based on these outcomes from VISION.
Since VISION, other data suggests that this treatment sequencing is safe. Sartor and colleauges in 20225 assessed 26 patients that received 177Lu-PSMA radioligand therapy after radium-223. These patients received radium-223 for a median of 6 injections and subsequently received 177Lu-PSMA radioligand therapy for a median of 3.5 months (>= the 4th line of therapy for 69% of patients). The median time between radium-223 and 177Lu-PSMA radioligand therapy was 8 months (range: 1-31 months), with a median overall survival of 28 months from the start of radium-223 and 13.2 months from the start of 177Lu-PSMA radioligand therapy.
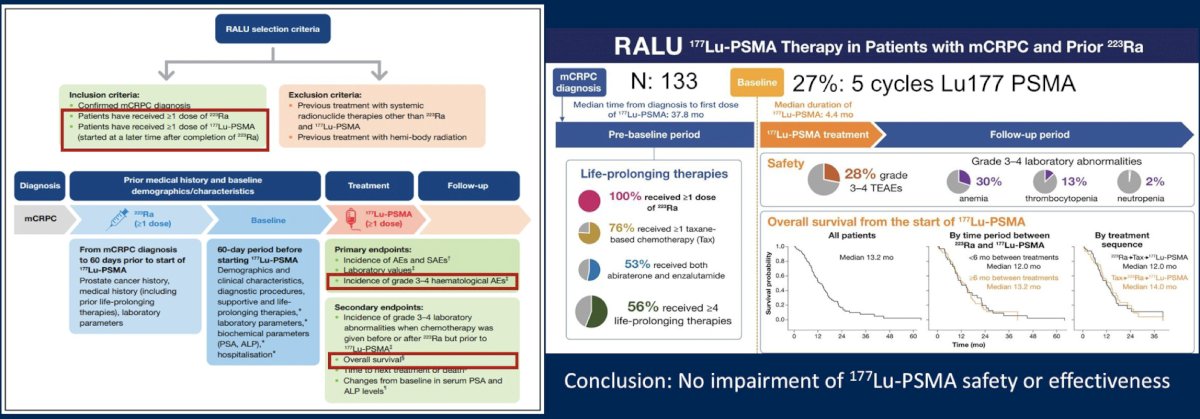
Dr. Dizdarevic also discussed the interim analysis of the RaLu study,4 published in 2023, showing that the median time between treatment with radium-223 and 177Lu-PSMA-617 therapy among 49 patients was 9.3 months (range: 0.9-41.9), with an acceptable toxicity given the grade 3-4 treatment emergent adverse event rate was 41%. The median overall survival from the first radium-223 injection was 31.4 months, and the overall survival from the first 177Lu-PSMA-617 injection was 12.6 months. Thus, in patients with bone-predominant disease, radium-223 before 177Lu-PSMA-617 treatment was clinically feasible and well tolerated, with a similar survival outcome to those reported in previous studies:
However, retrospective studies have inherent limitations with the risk of selection bias based on clinical judgement or preference.
For timing of treating with 177Lu-PSMA-617 after radium-223, this can be initiated as early as 8 weeks after progression on radium-223 in mCRPC patients. Baumgarten et al.7 showed an observed progression free survival of 10 months and overall survival of 18 months, and efficacy of 177Lu-PSMA-617 in mCRPC patients who have progressed on radium-223. In VISION, the median imaging-based progression free survival was 8.7 months, and the median overall survival was 15.3 months in the 177Lu-PSMA-617 arm. Baumgarten et al. also showed that the hematological safety profile of 177Lu-PSMA-617 treatment within 8 weeks of radium-223 therapy was consistent with that seen in the VISION trial. There was an increased incidence of significant hematological adverse events in patients with advanced disease and diffuse involvement, but there was no significant nephrotoxicity that occurred.
In the WARMTH study8 published in 2021, Ahmadzadehfar and colleagues noted that prior radium-223 among those patients with subsequent 177Lu-PSMA-617 radioligand therapy had a positive impact on overall survival, with the effect significant in two subgroups:
- 6-20 lesions: overall survival was 16.4 months versus 12.1 months, HR 1.58 (95% CI 1.0-2.4, p = 0.038)
- Diffuse involvement: overall survival was 11.0 months versus 7.1 months, HR 1.39, 95% CI 1.0-1.9, p = 0.034)
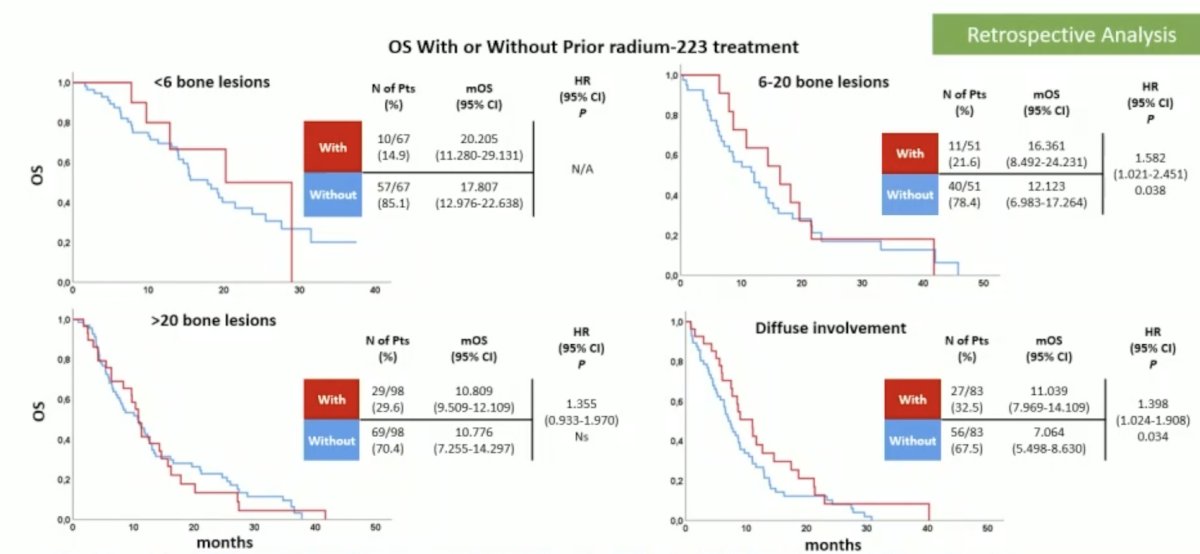
However, in this study, overall survival of all patients negatively correlated with the extent of bone involvement.
Regarding combination treatments, there are many unanswered questions as to why, when, and how to use combined targeted radionuclides and/or targeted radionuclides with non targeted radionuclide treatments. What about tandem or cocktail approaches to combination treatments?
- Dual-isotope combinations, or tandems or cocktail approaches, may improve tolerability while retaining a high tumor dose
- The same radiobiologic properties that make 225Ac-PSMA therapeutically potent also contribute to a higher incidence of severe toxicities (ie. xerostomia, making the salivary glands a key dose-limiting agent)
- Xerostomia from 177Lu-PSMA-617 is often temporary; however, with 225Ac-PSMA there is a greater incidence of xerostomia, which can significantly diminish patient quality of life and lead to treatment discontinuation
Dr. Dizdarevic then discussed the phase I/II ongoing ALPHABET trial, which is testing the combination of 177Lu-PSMA-I&T + radium-223. The hypothesis is that radium-223 in combination with 177Lu-PSMA-I&T leads to deeper and more durable response. Patients will receive 177Lu-PSMA-I&T 7.4 GBq IV every 6 weeks + radium-223 IV every 6 weeks for up to 6 cycles/doses. The co-primary objective is to determine the maximum tolerated dose of radium-223 when combined with 177Lu-PSMA-I&T, and the PSA50 rate. Secondary objectives include adverse events, efficacy through radiographic and PSA progression free survival, overall survival, and objective response rate, as well as evaluation of pain and health related quality of life.
Dr. Dizdarevic notes that harnessing the potential of dual-targeting radiopharmaceuticals in Nuclear Medicine is a British Nuclear Medicine Society strategy high impact goal.
Dr. Dizdarevic concluded her presentation discussing sequencing and combining beta and alpha targeted radionuclide treatments in the management of patients with prostate cancer with the following take home points:
- Prostate cancer is a heterogeneous disease with a potential phenotypic shift
- Therapies in prostate cancer, including radiopharmaceuticals are sequenced to provide patients the opportunity to receive as many life-prolonging therapies as possible
- Sequencing alpha and beta theranostic options in prostate cancer treatment is proving to be safe in clinical practice; however, combination or concomitant treatments require further research
- Multi-tracer imaging for prostate cancer patient selection for treatment can personalize treatment, directing toward the most appropriate targeted treatment (ie. either sequencing or in combination treatment)
Presented by: Sabina Dizdarevic, University Hospitals Sussex NHS Foundation Trust, Brighton & Sussex Medical School, University of Sussex and Brighton, Brighton, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting, New Orleans, LA, June 21st – 24th, 2025
References:
- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369(3):213-223.
- Harmon SA, Mena E, Shih JH, et al. A comparison of prostate cancer bone metastases on 18F-sodium fluoride and Prostate Specific Membrane Antigen (18F-PSMA) PET/CT: Discordant uptake in the same lesion. Oncotarget. 2018 Dec 28;9(102):37676-37688.
- Uprimmy C, Svirydenka A, Fritz J, et al. Comparison of 68Ga-PSMA-11 PET/CT with 18F-NaF- PET/CT in the evaluation of bone metastases in metastatic prostate cancer patients prior to radionuclide therapy. Eur J Nucl Med Mol Imaging. 2018 Oct;45(11):1873-1883.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Sartor O, la Faougere C, Essler M, et al. 177Lu-Prosate-Specific Membrane Antigen ligand after 223Ra Treatment in Men with Bone-Metastatic Castration-Resistant Prostate Cancer: Real-World Clinical Experience. J Nucl Med. 2022 Mar;63(3):410-414.
- Rahbar K, Essler M, Pabst KM, et al. Safety and Survival Outcomes of 177Lu-Prostate-Specific Membrane Antigen Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer with Prior 223Ra Treatment: The RALU Study. J Nucl Med. 2023 Apr;64(4):574-578.
- Baumgarten J, Groener D, Ngoc CN, et al. Safety and efficacy of 177Lutetium-PSMA-617 Radioligand Therapy Shortly after Failing 223Radium-Dichloride. Cancers (Basel). 2022 Jan 22;14(3):557.
- Ahmadzadehfar H, Matern R, Baum RP, et al. The impact of the extent of bone involvement on overall survival and toxicity in mCRPC patients receiving [177Lu]Lu-PSMA-617: A WARMTH multicentre study. Eur J Nucl Med Mol Imaging. 2021 Nov;48(12):4067-4076.