(UroToday.com) The 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting held in New Orleans, LA, was host to a Radiopharmaceutical Therapy Trials with Dosimetry session. Dr. Angela Jia presented the STARLiT trial of stereotactic body radiotherapy (SBRT) plus 177Lu PSMA-617 in patients with locally advanced prostate cancer.
The majority of incident prostate cancer diagnoses (85%) are non-metastatic at presentation, and among these non-metastatic tumors, 30% are considered to be high- or very high-risk tumors.

The current treatment recommendations for patients with high- or very high-risk prostate cancer, including locally advanced, include external beam radiotherapy (5–45 treatments) plus 18–36 months of ADT +/- abiraterone/prednisone for patients meeting the STAMPEDE eligibility criteria.1 However, this treatment paradigm is associated with significant morbidity, including:
- ≥35% Grade ≥3 toxicity
- Time to testosterone recovery ≥5 years
- ≥40% of patients never fully recover testosterone
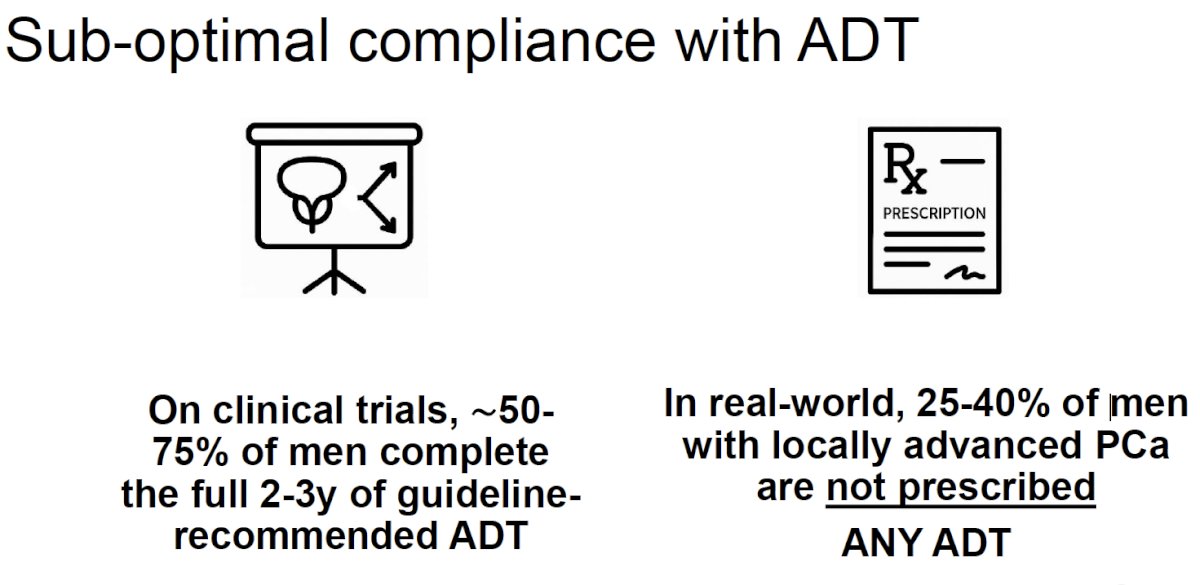
Furthermore, patients tend to be non-compliant with ADT regimens. In a clinical trial setting, only 50-75% of patients complete the fully recommended 2–3-year course of ADT. Furthermore, 25-40% of men with locally advanced prostate cancer are not prescribed any ADT in the real-world.
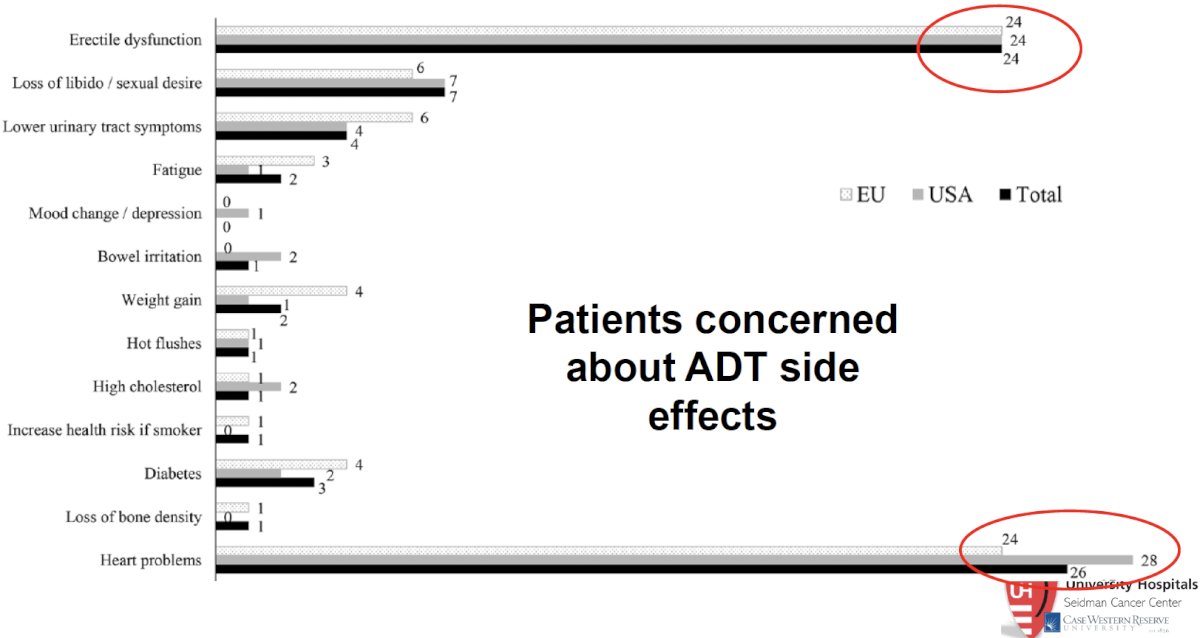
Potential reasons for this non-compliance/underutilization of ADT include patient concerns regarding the known side effects of ADT, namely erectile dysfunction and cardiovascular disease.
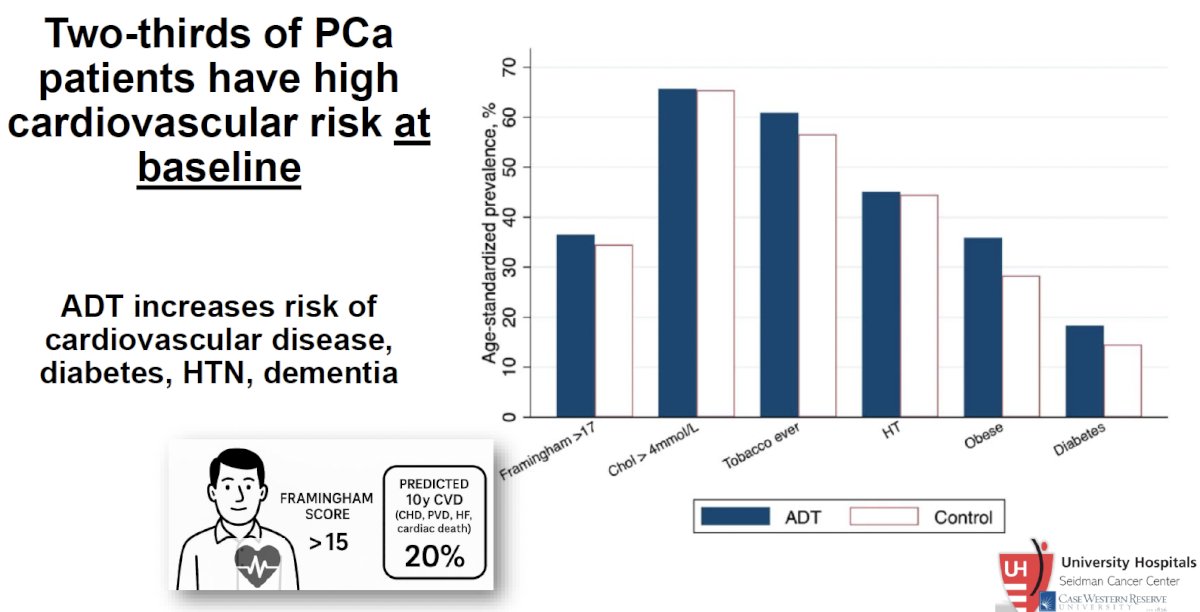
These concerns are particularly relevant given that two-thirds of prostate cancer patients have high cardiovascular risk at baseline, with ADT increasing the risk of cardiovascular disease, diabetes, hypertension, and dementia.
These concerns and challenges have led to the evaluation of shorter durations of intensified systemic therapy (e.g., AASUR, ASCLEPIUS, FORMULA-509 trials). However, the evaluation of alternative, non-hormonal approaches has also gained interested in this disease space.
177Lu-PSMA-617 is currently approved by the US Food and Drug Administration (FDA) for the treatment of metastatic castration-resistant prostate cancer (mCRPC) patients who have been treated with an androgen receptor pathway inhibitor (ARPI) and taxane-based chemotherapy (VISION and TheraP)2 or are considered appropriate to delay taxane-based chemotherapy (PSMAfore).3
STARLiT is a phase I/II trial that is evaluating SBRT + 177Lu-PSMA-617 in patients with newly diagnosed very high-risk prostate cancer, defined by ≥2 of the following:
- cT3
- ≥GG4
- PSA ≥40 ng/ml
- cN1
Eligible patients must have PSMA PET positive disease with an SUVmax ≥10 and no evidence of metastatic disease.

Eligible patients (n=45) will receive 177Lu-PSMA-617 followed by SBRT to the prostate and nodes 6 weeks later, and then 177Lu-PSMA-617 cycles every 6 weeks thereafter with the total number of planned cycles dependent upon dose-limiting toxicities. SPECT/CT imaging will be performed 48 and 72 hours following the initial 177Lu-PSMA dose and at 72-hour intervals following subsequent 177Lu-PSMA doses.
The primary endpoint for the phase I portion is the maximally tolerated dose of Lu-PSMA when administered with prostate SBRT, and the 3-year ADT-free survival for the phase II portion. Secondary endpoints include:
- Overall survival
- Cumulative incidence of distant metastases and prostate cancer-specific survival
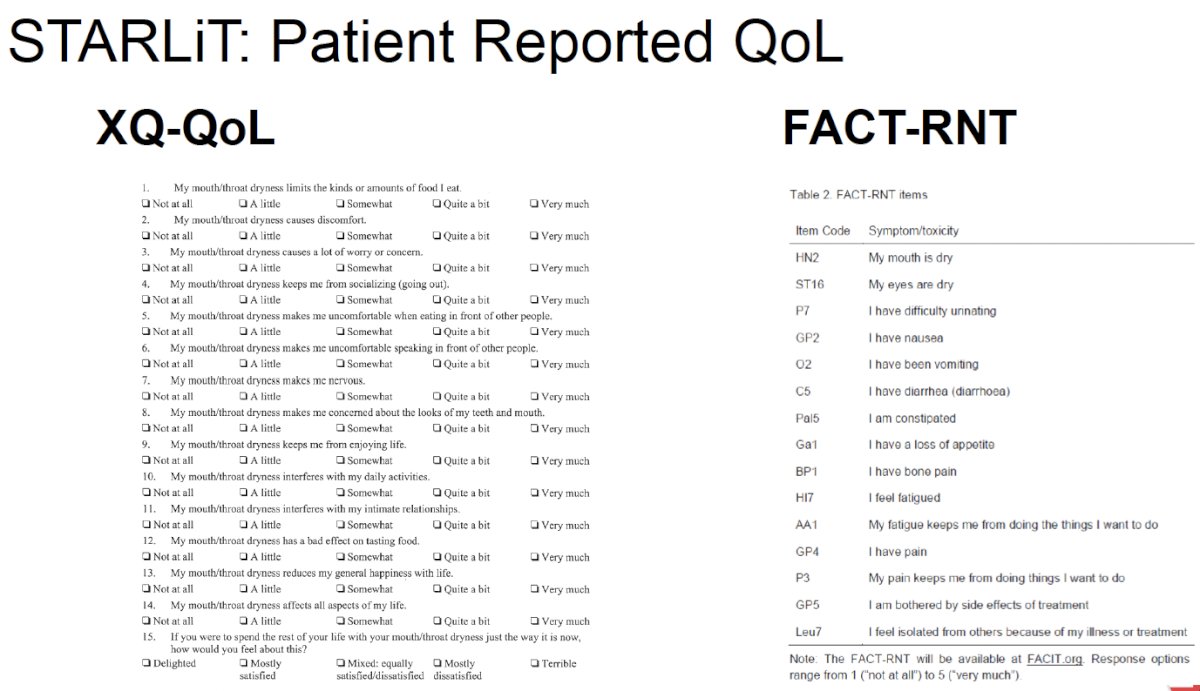
- Patient reported quality of life, assessed using the XQ-QoL and FACT-RNT questionnaires
- Time to salvage therapy
Dr. Jia concluded her presentation of the STARLiT trial as follows:
- The current standard of care for patients with localized or locally advanced high/very high-risk prostate cancer remains external beam radiotherapy + long-term ADT +/- an androgen receptor pathway inhibitor
- This is associated with significant toxicity, especially given that approximately two-thirds of newly diagnosed prostate cancer patients are at high risk of cardiovascular disease
- STARLiT evaluates an ADT-free approach, which combines two cytotoxic therapies, 177Lu-PSMA + SBRT, in locally advanced prostate cancer
- Open questions remain:
- Dosimetry – absorbed dose?
- Ideal number of cycles?
- Is there synergy with external beam radiotherapy?
- Are there predictive biomarkers to adapt treatment?
- Multidisciplinary care is essential – collaboration between nuclear medicine, medical oncology, and radiation oncology is key
Presented by: Angela Jia, MD, PhD, Assistant Professor, Department of Radiation Oncology, Case Western Reserve University, University Hospitals Cleveland Medical Center, Cleveland, OH
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting, New Orleans, LA, June 21st – 24th, 2025
References:
- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomized controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022; 399(10323):447-460.
- U.S. Food and Drug Administration. FDA approves Pluvicto for metastatic castration-resistant prostate cancer. 2022 Mar 23. Accessed 2025 Jun 22. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pluvicto-metastatic-castration-resistant-prostate-cancer
- U.S. Food and Drug Administration. FDA expands Pluvicto’s metastatic castration-resistant prostate cancer indication. 2025 Mar 28. Accessed 2025 Jun 22. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-expands-pluvictos-metastatic-castration-resistant-prostate-cancer-indication