(UroToday.com) The 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting held in New Orleans, LA, was host to a session on non-beta emitter PSMA radioligand therapy. Dr. Machaba Sathekge discussed the use of Actinium-225 (225Ac) for the treatment of advanced prostate cancer.
Dr. Sathekge highlighted that the 225Ac market is poised for significant growth, driven by increasing interest in targeted alpha therapies for advanced cancers, including prostate cancer. Both Verified Market Research and Valuates Reports project compound annual growth rates of approximately 15% through 2031, with the market value expected to surge from a modest $0.7 million in 2023 to $1.7–1.8 billion by 2031.


It is clear that the clinical ‘footprint’ of 225Ac therapy is growing across a range of malignancies. The left panel below details patient cohorts treated with radioconjugates in various cancers, highlighting prostate cancer as the leading clinical indication, with 190 patients receiving [225Ac]PSMA-617. Other malignancies under investigation include leukemia, lymphoma, neuroendocrine tumors, glioma, and bladder cancer, demonstrating broadening applicability.
The right panel illustrates the decay chain of 225Ac, emphasizing its therapeutic potency via a cascade of α-emissions (each 5.8–8.4 MeV) through intermediates such as 221Fr, 217At, and 213Bi. These high-energy emissions are central to inducing lethal double-strand DNA breaks in tumor cells, while the relatively short range of α-particles helps spare surrounding healthy tissue.

Dr. Sathekge dubbed 225Ac “the world’s rarest drug’, and there are ongoing global efforts to increase production to better meet the global demand for this agent.

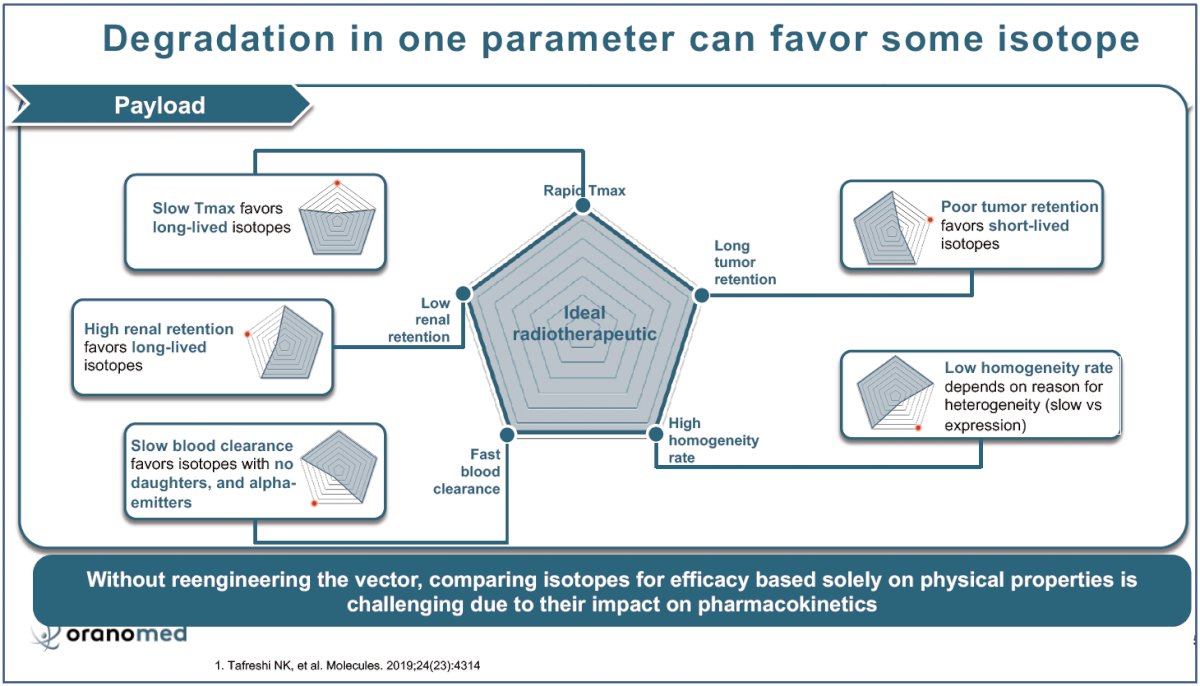
The diagram below highlights a key challenge in radiopharmaceutical design: the interplay between vector pharmacokinetics and radionuclide selection. The central “ideal radiotherapeutic” profile balances five key parameters—rapid Tmax, low renal retention, long tumor retention, fast blood clearance, and high target homogeneity.
However, degradation in any one of these parameters shifts the advantage toward specific isotope classes:
- Slow Tmax or high renal retention favors long-lived isotopes to allow sufficient residence time.
- Poor tumor retention or low homogeneity may paradoxically benefit from short-lived isotopes to avoid unnecessary off-target toxicity.
- Slow blood clearance favors isotopes without radioactive daughters (e.g., 213Bi), particularly alpha-emitters, to minimize systemic exposure.
Crucially, the figure drives home a critical translational insight: without reengineering the vector, comparing isotopes based on physical half-life or emission alone is misleading. The biological context—specifically, the pharmacokinetics of the carrier molecule—must guide radionuclide selection.
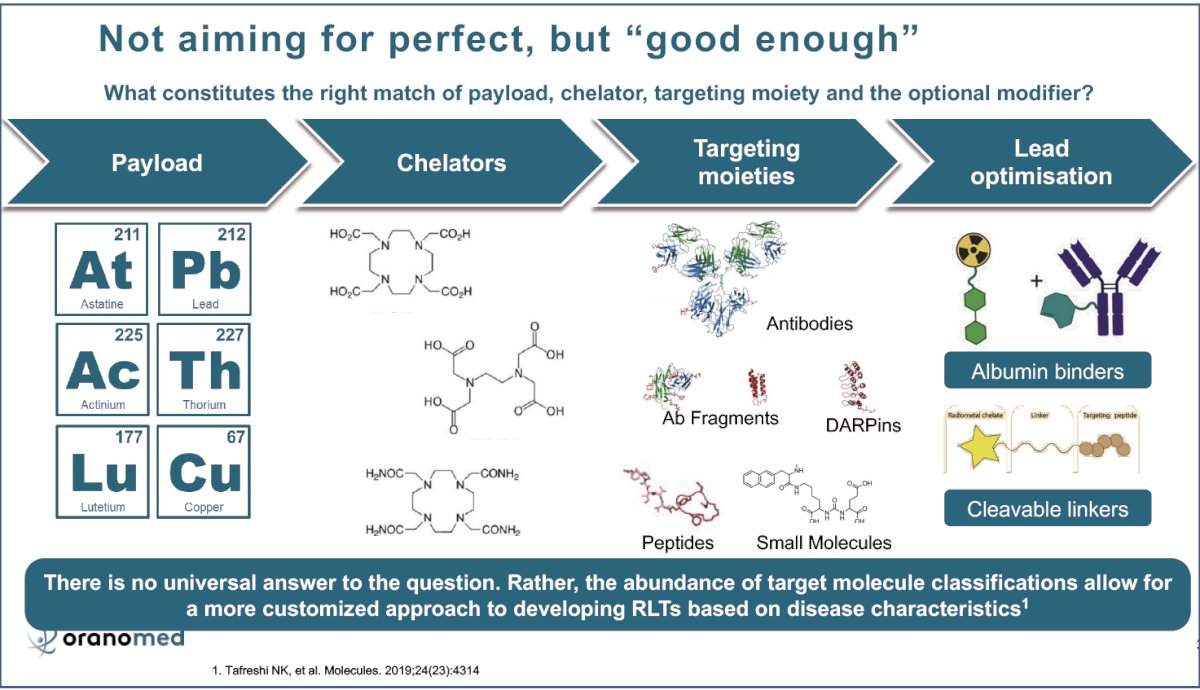
Dr. Sathekge argued that a pragmatic approach in radioligand therapy development is needed, rather than a one-size-fits-all solution. This strategy emphasizes a modular, disease-specific approach integrating four key elements: payload, chelator, targeting moiety, and lead optimization.
Payload selection spans alpha- and beta-emitters (e.g., 211At, 225Ac, 212Pb, 177Lu), while chelators (e.g., DOTA, macropa derivatives) ensure stable radionuclide complexation. A range of targeting moieties—from full antibodies and fragments to DARPins, peptides, and small molecules—enables flexibility across cancer types with different biology and accessibility. The final layer, lead optimization, introduces optional modifiers like albumin binders to enhance plasma half-life or cleavable linkers for tumor-selective payload release.
α-emitters have a high linear energy transfer (LET) with a submillimeter range, which is ideal for producing localized damage. They create potent doubled-stranded DNA breaks, mitochondrial oxidative stress, and cytokine release. These lead to direct tumor cell death while minimizing collateral damage to surrounding tissue. Dr. Sathekge noted that the field is moving toward embracing the indirect effects that α-emitters trigger:
- Bystander effects (RIBE) and immune activation can result in abscopal effects (AbsE)—tumor shrinkage at distant, non-irradiated sites.
- The inset highlights how α-induced crossfire effects (CF), RIBE, and AbsE overlap and expand the therapeutic radius beyond the emitter’s physical range.

The figure below highlights the recoil and redistribution of daughter nuclides following the decay of Actinium-225, and how internalization impacts safety and efficacy.
In the left panel, we see two scenarios:
- In internalizing vectors, once ²²⁵Ac binds its target and is internalized, its daughter nuclides (like ²¹³Bi) remain mostly trapped intracellularly, allowing for localized, high-LET DNA damage—ideal for therapeutic effect.
- In contrast, with non-internalizing vectors, the high recoil energy from α-decay causes daughter isotopes to escape, leading to off-target toxicity as these short-lived particles redistribute systemically (especially ²¹³Bi, ²¹¹At, and ²⁰⁹Pb).
- The right panel reinforces this by illustrating how the internalization of targeted-alpha therapy pharmaceuticals results in precise tumor irradiation, while a lack of internalization increases the risk of healthy tissue irradiation due to circulating daughters.
- Optimizing vector internalization can mitigate toxicity and enhance tumor kill, which is paramount for advancing the safety of alpha therapies like ²²⁵Ac-PSMA.

A fundamental challenge in targeted-alpha therapy with 225Ac remains the in vivo redistribution of daughter isotopes, namely Bismuth-213 (213Bi) and Francium-221 (221Fr), over time. The biodistribution of these daughter radionuclides does not mirror that of the parent compound, 225Ac. This introduces unintended off-target irradiation—especially in the kidneys—and highlights the critical need for chelators that retain daughter nuclides and internalizing vectors to minimize systemic escape.

In an attempt to overcome these challenges, there have been ongoing efforts to improve the targeted delivery of 225Ac to tumor cells. AKY-1189 is a novel, first-in-class miniprotein radiopharmaceutical designed to deliver 225Ac to Nectin-4 expressing tumors, including triple-negative breast cancer—a notoriously aggressive subtype with limited treatment options.

Dr. Sathekge noted that there are numerous ongoing trials evaluating 225Ac-PSMA therapy in the metastatic (mostly castration-resistant) prostate cancer space, as summarized in the table below:

How does 225Ac fit into the current treatment landscape of advanced prostate cancer? In 2024, Dr. Sathekge and colleagues published the results of WARMTH Act, a worldwide multicenter retrospective study of 488 mCRPC patients who received ≥1 cycle of 225Ac (8 MBq) between January 2016 and May 2023. This was a heavily pre-treated patient cohort with previous lines of therapy including docetaxel (66%), cabazitaxel (21%), abiraterone (39%), enzalutamide (39%), 177Lu-PSMA (32%), and 223Ra (4%). The median baseline PSA was 170 ng/mL. At a median follow-up duration of 9 months, the median overall survival was 15.5 months, and the median progression-free survival was 7.9 months.1

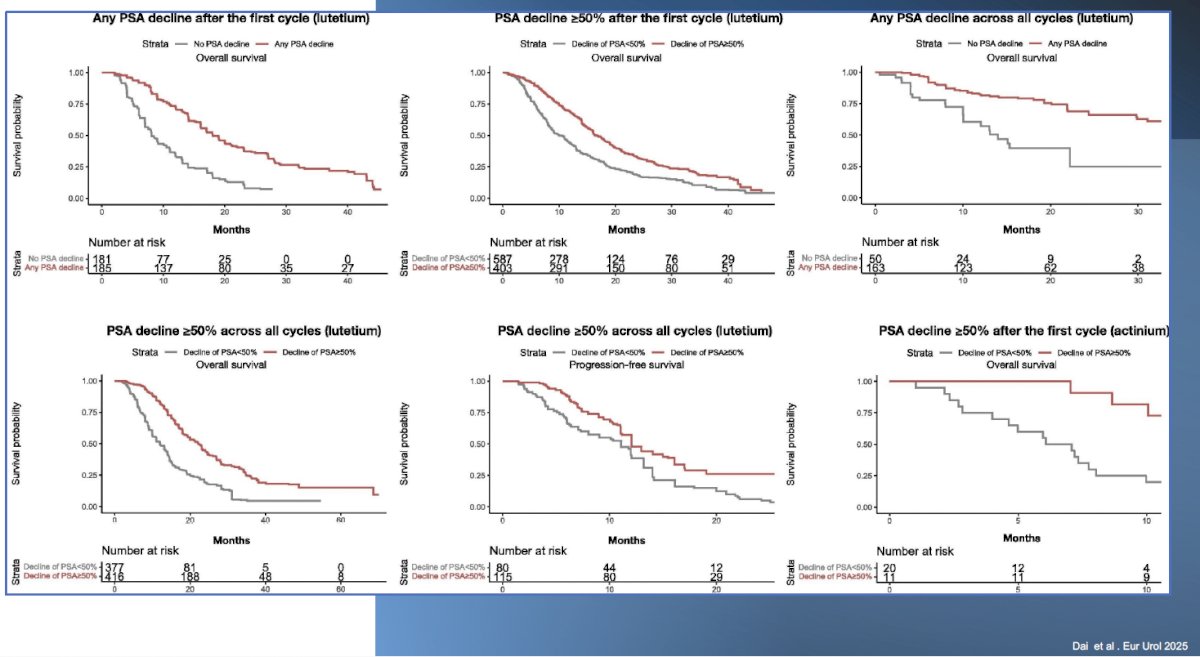
Dr. Sathekge highlighted the important prognostic significance of early PSA responses for patients treated with radionuclide therapy – both 177Lu and 225Ac, even after the 1st cycle. As summarized in the Kaplan-Meier curves below, patients with any or ≥50% PSA decline after the 1st or all cycles of 177Lu or 225Ac therapy had superior overall survival outcomes, compared to those that did not achieve such PSA responses.2
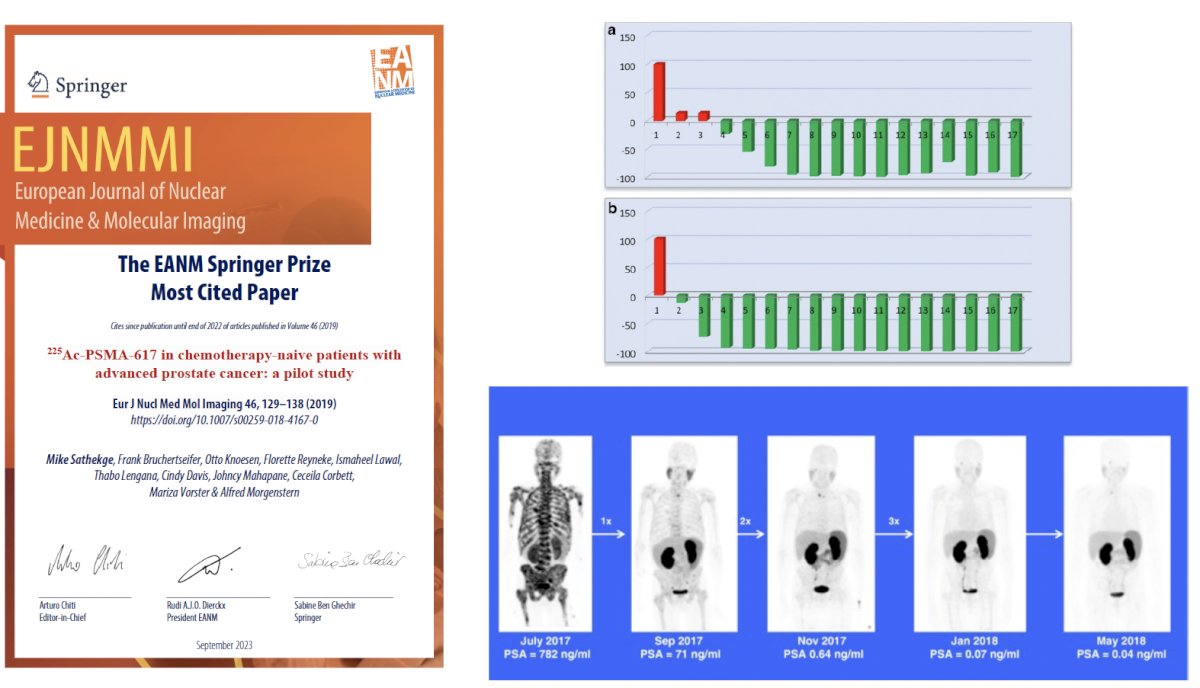
In the chemotherapy-naïve setting, Dr. Sathekge and colleagues published the results of an analysis of 17 patients with advanced prostate cancer receiving 225Ac therapy in 2019. Good antitumor activity assessed by serum PSA level and 68Ga-PSMA-PET/CT was seen in 16/17 patients. In 14/17 patients, PSA decline ≥90% was seen after treatment, including seven patients with undetectable serum PSA following two (2/7) or three cycles (5/7) cycles of 225Ac-PSMA-617. Fifteen of 17 patients had a > 50% decline in lesion avidity for tracer on 68Ga-PSMA-PET/CT, including 11 patients with complete resolution (PET-negative and either stable sclerosis on CT for bone or resolution of lymph node metastases) of all metastatic lesions.3
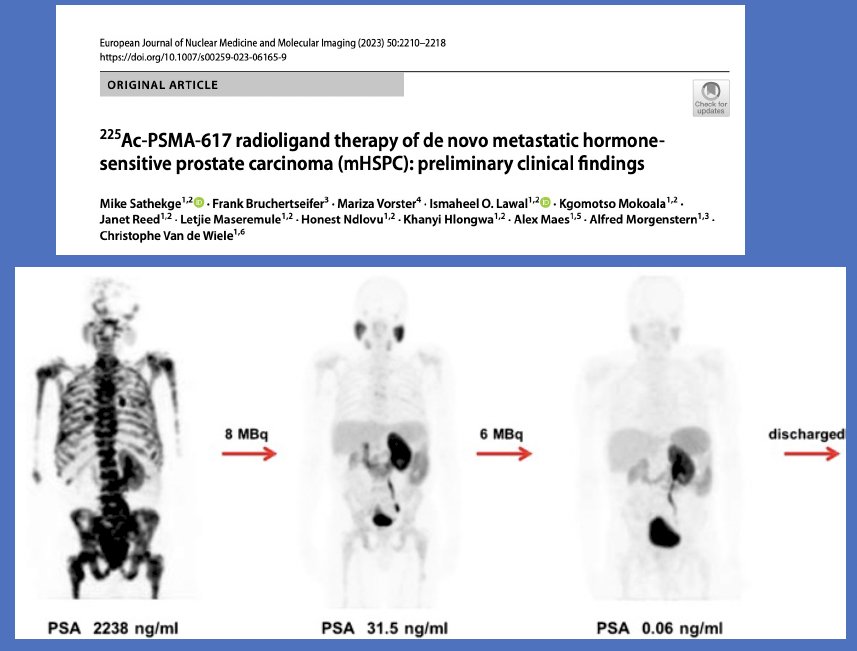
Moving 225Ac further up the ‘treatment chain’, in 2023, Dr. Sathekge and colleagues published the preliminary clinical findings of 225Ac-PSMA-617 radioligand therapy in patients with metastatic hormone-sensitive prostate cancer (mHSPC).4 Twenty-one mHSPC patients received 225Ac-PSMA-617 radioligand therapy, and twenty (95%) experienced any decline in PSA, with 18 (86%) experiencing a PSA decline ≥50%. 4/21 patients achieved undetectable PSA levels. Overall, administration of 225Ac-PSMA-617 was well tolerated. The commonest toxicity seen was grade I/II dry mouth, observed in 94% of patients
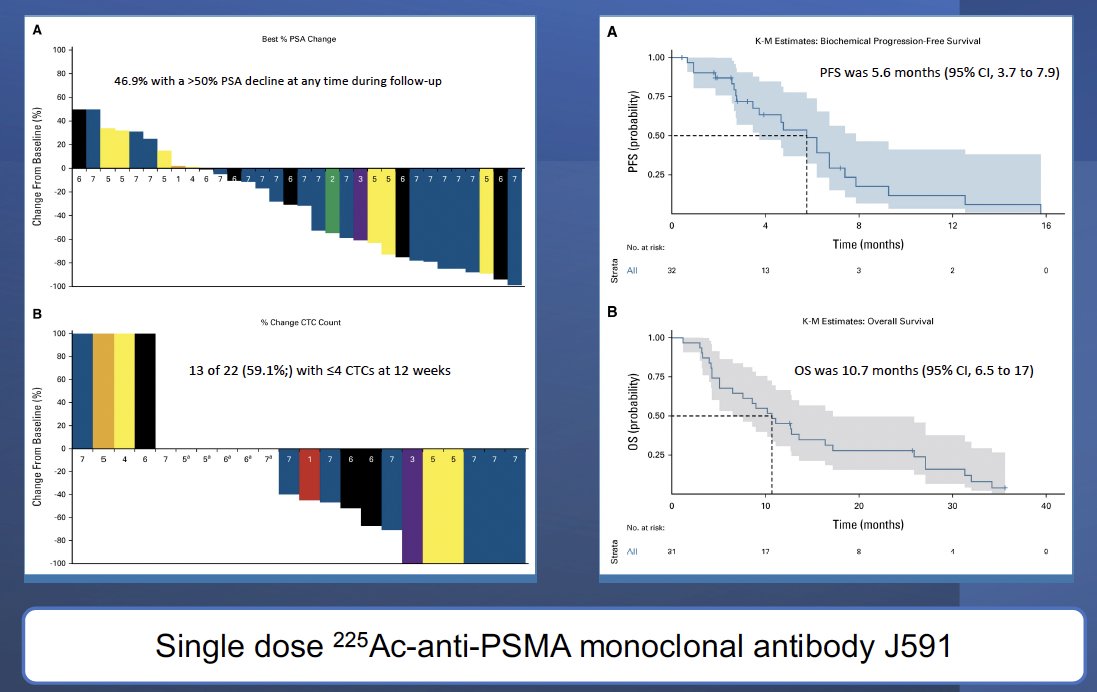
Tagawa et al. have demonstrated that promising treatment efficacy can be achieved with a single dose of 225Ac-anti-PSMA monoclonal antibody J591. Thirty-two patients with progressive mCRPC received 225Ac-J591 in an accelerated dose-escalation design. PSA declines and circulating tumor cell (CTC) control were observed: 47% had a ≥50% PSA decline at any time, and protocol-defined CTC count responses occurred in 13 of 22 (59%) patients.5
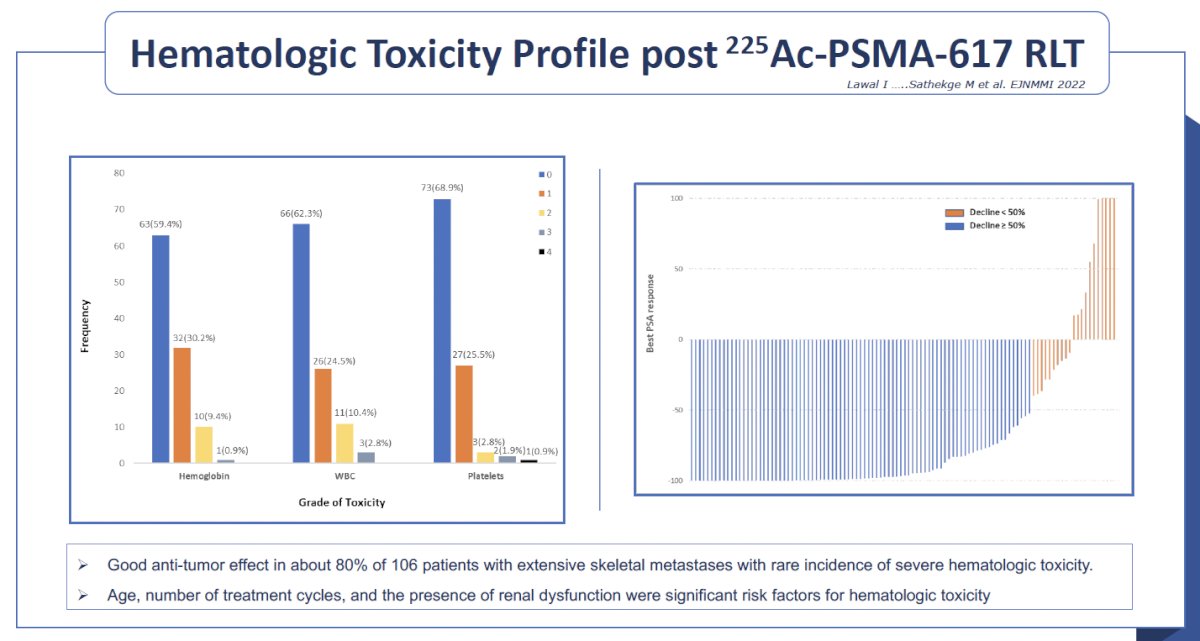
Dr. Sathekge acknowledged the high incidence of bone marrow and hematologic toxicity with 225Ac and questioned whether we will be able to combine 225Ac with 177Lu therapy in future studies given this overlapping toxicity profile, while maintaining their combined therapeutic effect.
Nonetheless, novel 225Ac combinations with immunotherapy (increased immunogenicity with targeted alpha therapy) and other radiopharmaceuticals with non-overlapping toxicities are currently being evaluated in ongoing studies.

Presented by: Machaba Michael Sathekge, MD, PhD, Professor, Head of Nuclear Medicine Department, University of Pretoria and Steve Biko Academic Hospital, Pretoria, South Africa
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting, New Orleans, LA, June 21st – 24th, 2025
References:
- Sathekge MM, Lawal IO, Bal C, et al. Actinium-225-PSMA radioligand therapy of metastatic castration-resistant prostate cancer (WARMTH Act): a multicentre, retrospective study. Lancet Oncol. 2024; 25(2): 175-83.
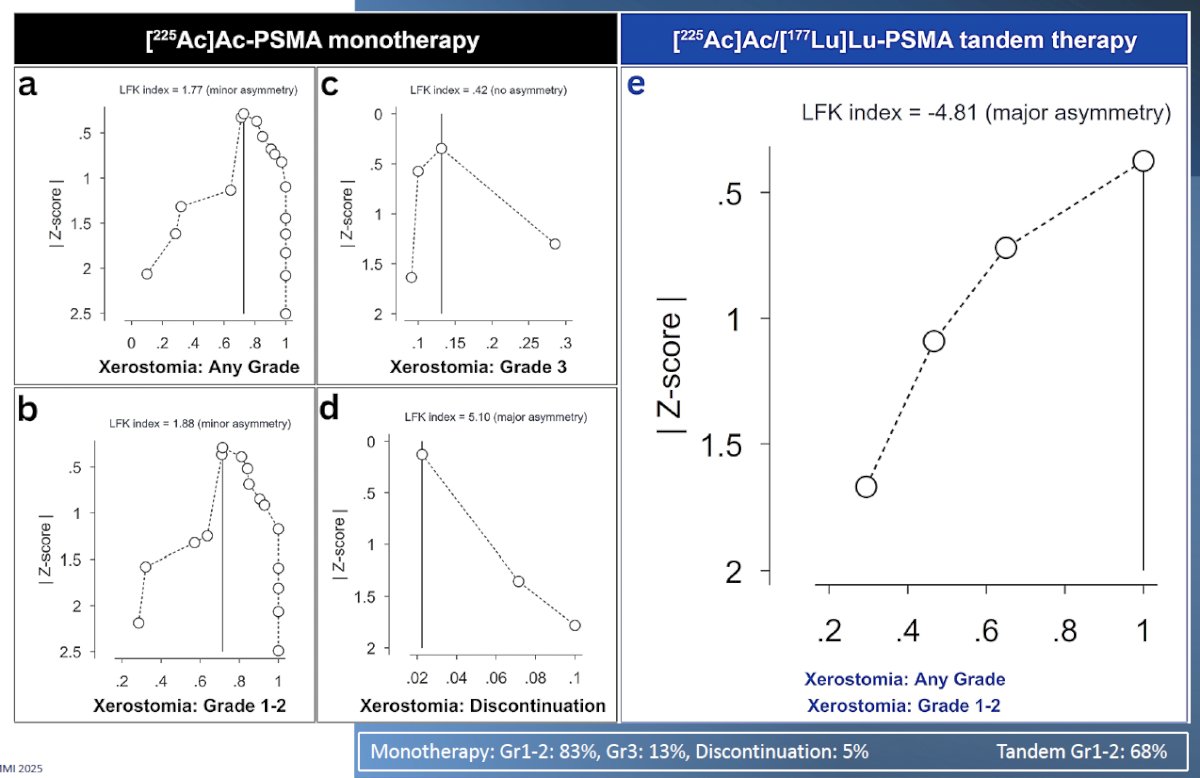
- Dai YH, Chen PH, Lee DJ, Andrade G, Vallis KA. A Meta-Analysis and Meta-Regression of the Efficacy, Toxicity, and Quality of Life Outcomes Following Prostate-Specific Membrane Antigen Radioligand Therapy Utilising Lutetium-177 and Actinium-225 in Metastatic Prostate Cancer. Eur Urol. 2025; 87(4): 398-408.
- Sathekge M, Bruchertseifer F, Knoesen O, et al. 225Ac-PSMA-617 in chemotherapy-naive patients with advanced prostate cancer: a pilot study. Eur J Nucl Med Mol Imaging. 2019; 46(1): 129-38.
- Sathekge M, Bruchertseifer F, Vorster M, et al. 225Ac-PSMA-617 radioligand therapy of de novo metastatic hormone-sensitive prostate carcinoma (mHSPC): preliminary clinical findings. Eur J Nucl Med Mol Imaging. 2023; 50(7): 2210-8.
- Tagawa ST, Thomas C, Sartor AO, et al. Prostate-Specific Membrane Antigen-Targeting Alpha Emitter via Antibody Delivery for Metastatic Castration-Resistant Prostate Cancer: A Phase I Dose-Escalation Study of 225Ac-J591. J Clin Oncol. 2024; 42(7): 842-51.