(UroToday.com) The 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting held in New Orleans, LA, was host to a session on non-beta emitter PSMA radioligand therapy. Dr. Tadashi Watabe discussed the use of Astatine-211 (211At) for the treatment of advanced prostate cancer.
211At is an emerging alpha-emitting nuclide with a half-life of 7.2 hours and is manufactured using a 30 MeV cyclotron with a natural bismuth target (209Bi+4He→211At+2n). ²¹¹At is produced through alpha irradiation of natural bismuth via the 209Bi(α,2n)211At reaction. A 29 MeV alpha particle beam (40 μA current) bombards a 75 mg/cm² bismuth target at a 15° incidence angle. With 1 hour of irradiation under optimized thermal and vacuum conditions, this setup yields approximately 1.3 GBq of ²¹¹At at the end of bombardment. To ensure beam stability and precise energy delivery, a beam wobbler (2 Hz, Φ3 mm) and a time-of-flight (TOF) detector monitor the beam at 29 ± 1% MeV. The bismuth target is maintained at 271.5°C with concurrent helium (30 L/min) and water (4 L/min at 5°C) cooling to dissipate heat and prevent target degradation.
²¹¹At decays via two primary mechanisms:
- Alpha emission (42%) with an energy of 5.9 MeV
- Electron capture (58%), resulting in the formation of 211Po, which subsequently undergoes alpha decay (7.5 MeV) to stable 207Pb
- This dual decay mechanism enables the delivery of high-linear energy transfer (LET) alpha particles, ideal for inducing double-strand DNA breaks in malignant cells, particularly in small cell clusters or single-cell micrometastases.
Alternative isotopes such as 210At are less favorable due to their decay to 210Po, which has known toxicity and a less favorable radiochemical profile. 211At, by contrast, decays safely to stable 207Pb, minimizing off-target radiation risk.

The global production sites for 211At are illustrated below. There are currently 5 production sites in Japan.

What are the physical characteristics of 211At and how does it compare to other α and β emitters? 211At has the shortest half-life (7.2 hours). It combines a high therapeutic effect with a ‘very low’ exposure to the surrounding tissues. It does not require isolation and can be given on an outpatient basis. It can be produced domestically using cyclotron manufacturing. Importantly, it can be used for imaging purposes as well.

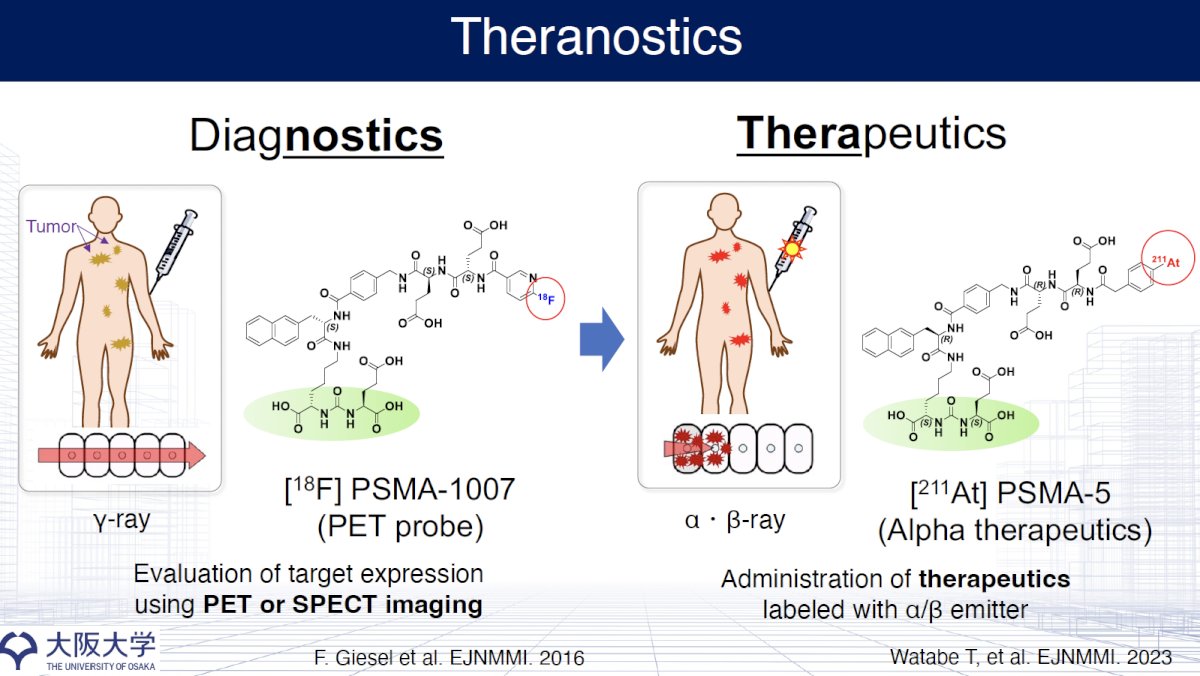
Theranostics continues to transform prostate cancer management through the dual application of imaging and therapy via molecular targeting. As illustrated, [¹⁸F]PSMA-1007 serves as a PET imaging probe enabling non-invasive evaluation of PSMA expression via PET or SPECT, identifying sites of metastatic disease. Once validated, therapeutic analogs such as [²¹¹At]PSMA-5—an alpha-emitting therapeutic—can be administered, delivering cytotoxic α- or β-emissions directly to PSMA-positive lesions.
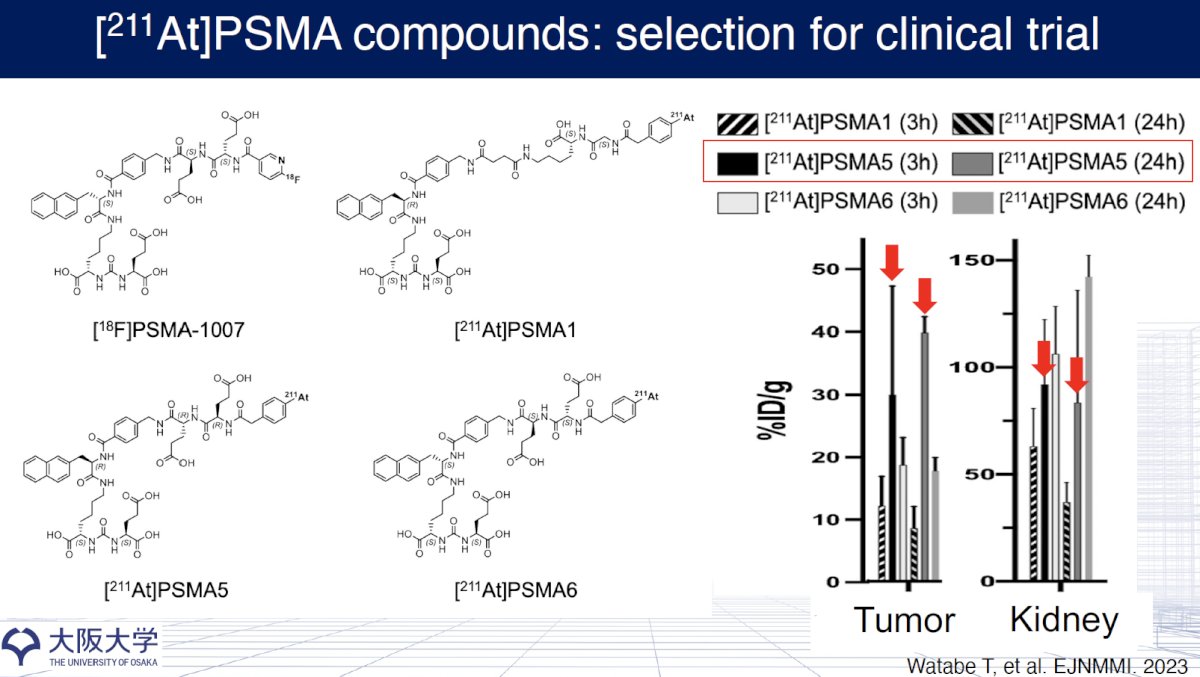
Various 211At-labeled PSMA compounds were compared for their tumor-targeting efficiency and renal uptake. This included [211At]PSMA1, [211At]PSMA5, and [211At]PSMA6, benchmarked against [18F]PSMA-1007. As shown in the figure, biodistribution studies (%ID/g) at 3 hours and 24 hours post-injection revealed that [211At]PSMA5 demonstrated the most favorable tumor uptake while maintaining relatively lower renal accumulation compared to other candidates, particularly at later time points (24h). These attributes suggest a superior tumor-to-kidney ratio, critical for minimizing nephrotoxicity in clinical application.
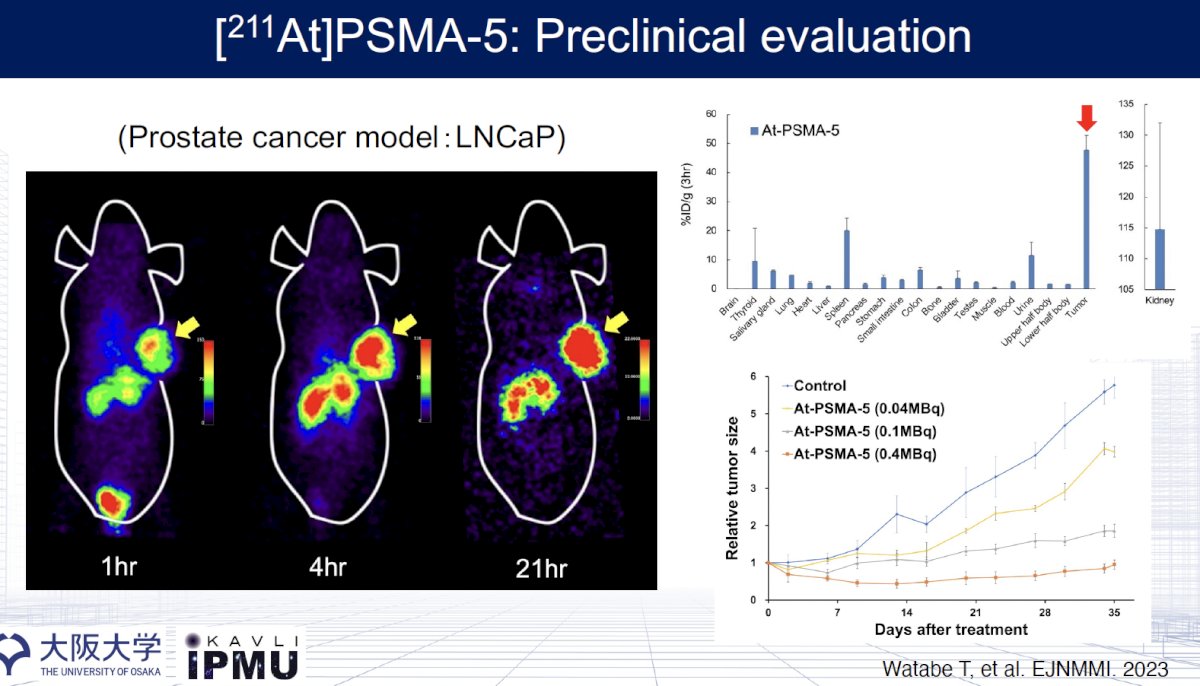
Serial SPECT imaging (1-, 4-, and 21-hours post-injection) shows persistent and intense tumor retention of [211At]PSMA5 (yellow arrows), confirming favorable in vivo pharmacokinetics.
Biodistribution analysis at 3 hours post-injection further supports high tumor specificity (%ID/g >130), with limited off-target uptake—particularly low accumulation in critical organs like the liver, lungs, and salivary glands. Notably, kidney uptake, a common concern in PSMA-targeted therapy, is moderate, underscoring a potentially safer therapeutic profile.
Dose-dependent tumor growth suppression is clearly demonstrated, with [211At]PSMA-5 at 0.4 MBq achieving near-complete tumor control by day 35 compared to controls. Even lower doses (0.1 MBq) showed substantial efficacy.1
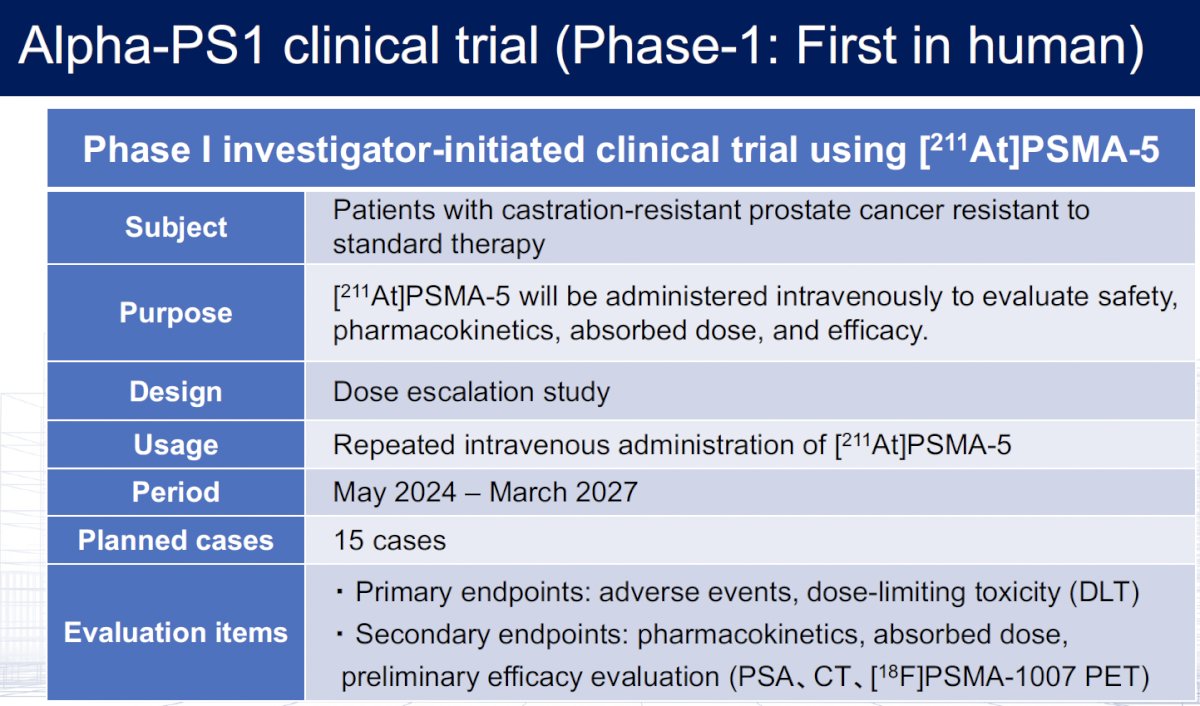
An ongoing investigator-initiated phase I dose-escalation trial is evaluating [211At]PSMA-5 in mCRPC patients. This trial will enroll 15 patients between May 2024 and March 2027 with primary endpoints of adverse events and dose-limiting toxicity.
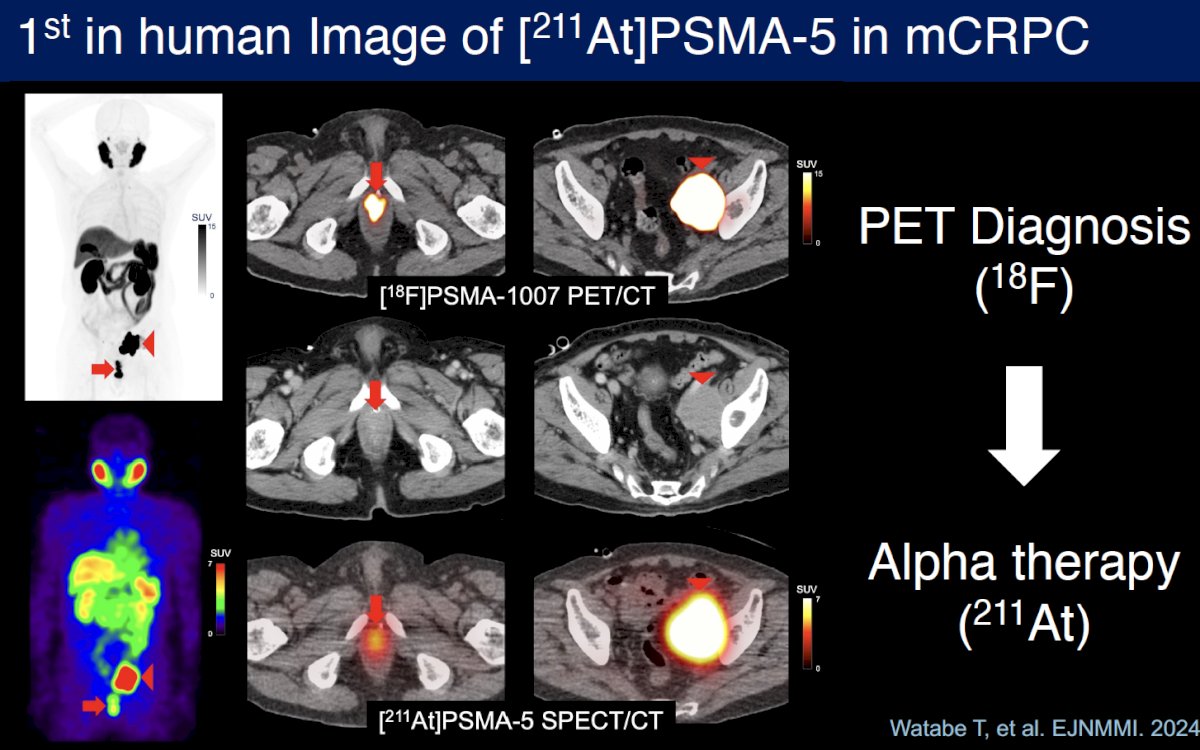
The first-in-human SPECT/CT image of [211At]PSMA-5 in a patient was reported by Watabe et al in 2024.2 [211At]PSMA-5 was administered to a man in his 70s with mCRPC refractory to standard treatment, including androgen receptor signaling inhibitors, docetaxel, and cabazitaxel. SPECT/CT imaging was performed 3 hours post-administration using a VERITON-CT (Spectrum Dynamics Medical) equipped with a full-ring cadmium zinc telluride (CZT) detector, targeting the 79 keV X-rays from the daughter nuclide of 211Po.
Pre-treatment [18F]PSMA-1007 PET/CT and [211At]PSMA-5 SPECT/CT images showed similar distribution patterns, with high uptake in recurrent/metastatic lesions. Both images revealed high accumulation in the soft tissue mass within the prostate area (SUVmax = 60.7 on [18F]PSMA-1007 PET and 4.9 on [211At]PSMA-5 SPECT) and in the enlarged left external iliac lymph node metastasis (SUVmax = 143.7 and 17.6, respectively). Physiological accumulation was similarly observed in both modalities in the salivary glands, liver, spleen, small intestine, and kidneys, with no detectable urinary excretion.
Presented by: Tadashi Watabe, MD, PhD, Associate Professor and Lecturer in the Department of Radiology at Osaka University, Osaka, Japan
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting, New Orleans, LA, June 21st – 24th, 2025
References:
- Watabe T, KanedaNakashima K, Shirakami Y, et al. Targeted αtherapy using astatine (^211At)labeled PSMA1, PSMA5, and PSMA6: a preclinical evaluation as a novel compound. Eur J Nucl Med Mol Imaging. 2023;50(3):849–858.
- Watabe T, Hatano K, Naka S, et al. First‑in‑human SPECT/CT imaging of [211At]PSMA‑5: targeted alpha therapy in a patient with refractory prostate cancer. Eur J Nucl Med Mol Imaging. 2025; 52(13):2253–2255.