(UroToday.com) At the 2021 Society of Nuclear Medicine & Molecular Imaging (SNMMI) Meeting’s Correlative Cross-Sectional and Molecular Imaging session, Dr. Jeremie Calais discussed the characterization of bone lesions in prostate cancer patients with PET/CT imaging.
Dr. Calais notes that the bone microenvironment is a biological target for PET imaging of bone metastasis, including the complex interplay between prostate cancer cells, osteolytic growth factors, bone-derived growth factors, osteoclasts, osteoblasts, bone marrow, cytokines and growth factors:

On the metastatic prostate cancer cell, there are additional receptors that have been characterized as targets for PET/CT imaging, including:
- SHBG for 18F-DHT
- PSMA for 68Ga-PSMA-11
- LAT1 for 18F-fluciclovine
- CTLs for 11C-choline
- GLUT1/GLUT2 for 18F-FDG
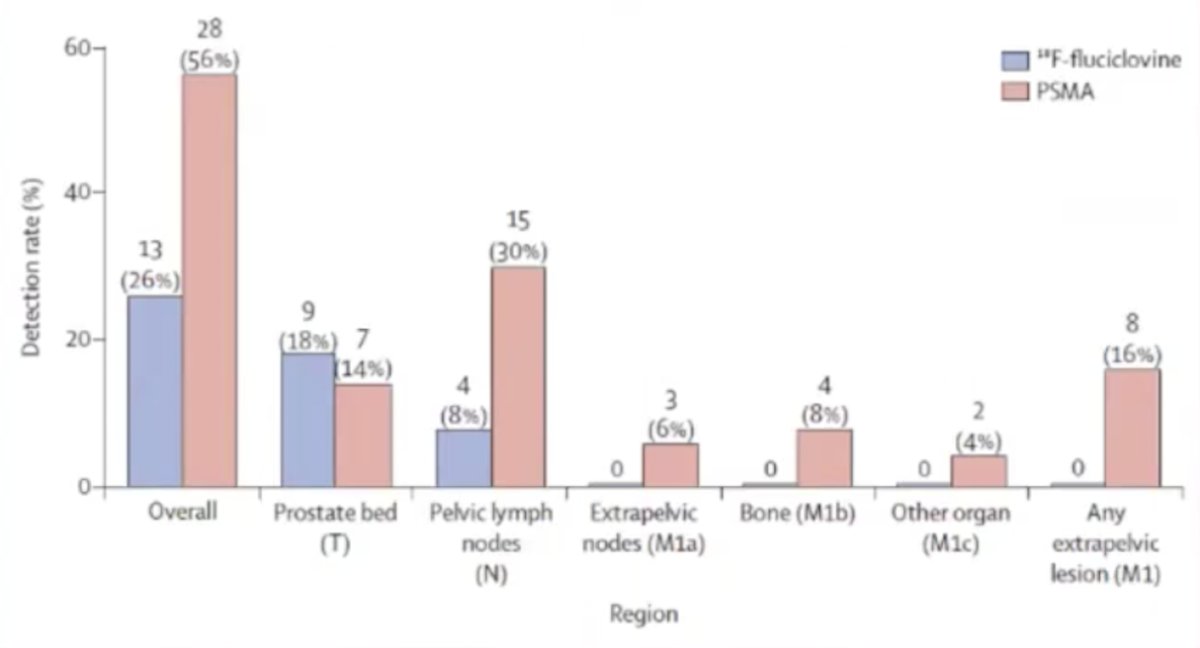
Currently, PSMA-PET is the most sensitive imaging modality for detecting prostate cancer metastases. A multitude of studies have demonstrated that PSMA PET/CT is superior to conventional imaging,1 PSMA PET/CT is superior to choline PET/CT, and PSMA PET/CT is superior to fluciclovine PET/CT.2 Dr. Calais then discussed in more detail the head-to-head comparison trial from his institution comparing 18F-fluciclovine and 68Ga-PSMA-11 PET/CT scans for localizing early biochemical recurrence of prostate cancer after radical prostatectomy. This study had 50 consecutive patients with biochemical recurrence and PSA levels ranging from ≥0.2 to ≤2.0 ng/mL without any prior salvage therapy. All patients underwent 18F-fluciclovine and 68Ga-PSMA-11 PET/CT scans within ≤15 days. PET/CT scans were each interpreted by three independent blinded expert readers not involved in study design and data acquisition. Region consensus interpretation (T, N, M1a, M1b, and M1c) was generated based on majority rule in cases of reader disagreement (2 versus 1). PET/CT scans were considered as positive if any region was rated as positive. Detection rates per-patient and per-region served as primary study endpoint. Secondary endpoints included detection rates stratified by PSA, sensitivity and positive predictive value verified by histopathology, clinical imaging and follow-up, and inter-reader agreement. The median age of patients was 68 years (IQR 64-74), and 22% of patients were N1. The median of the last PSA before PET/CT was 0.48 ng/mL (IQR 0.38-0.83) The median time interval between the 2 scans was 6 days (range 1-15). The detection rates were significantly lower with 18F-fluciclovine PET/CT than with 68Ga-PSMA-11 PET/CT per-patient (26% vs 56%; p = 0.003) and per-region for pelvic nodes (8% vs 30%; p = 0.003) or any extra-pelvic lesions (0% vs 16%; p = 0.008):
Reader agreement for 68Ga-PSMA-11 PET/CT image interpretations was significantly higher than for 18F-fluciclovine PET/CT (0.67 vs 0.20; p = 0.002). In patients with PSA levels from 0.2-0.5 ng/mL, 0.5-1.0 ng/mL, and 1.0-2.0 ng/mL, detection rates were 7/26 (27%), 5/18 (28%), and 1/6 (17%) with 18F-fluciclovine PET/CT, and 12/26 (46%), 12/18 (67%), and 4/6 (67%) with 68Ga-PSMA-11 PET/CT, respectively. Per patient sensitivity was 33% (95%CI 15-58%) and 66% (95%CI 42-85%) for 18F-fluciclovine PET/CT and 68Ga-PSMA-11 PET/CT, respectively (OR 3.5, 95% CI 0.67-34.5).
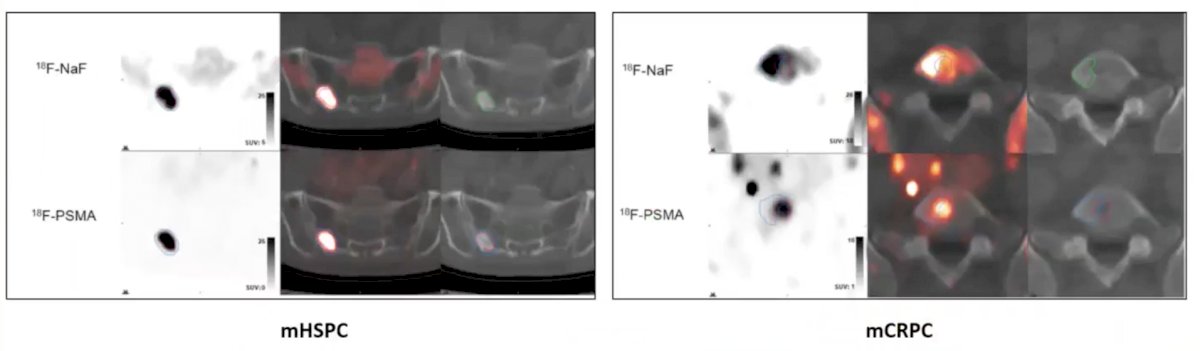
When looking at PSMA PET/CT versus F-Na PET/CT, Dr. Calais notes that Harmon et al.3 assessed the spatial concordance of 18F-NaF PET/CT and 18F-PSMA-targeted PET/CT among 19 patients with 149 prostate cancer bone metastatic lesions. Qualitatively, lesions exhibited a heterogeneous range of spatial concordance between PSMA and NaF uptake from completely matched to completely discordant. Quantitatively, overlap volume decreased as a function of tracer intensity and disease status, where lesions from patients with castration sensitive disease showed higher spatial concordance, while castration-resistant lesions demonstrated more frequent spatial discordance:
Currently, 68Ga-PSMA-11 PET/CR is FDA approved at UCLA and UCSF (December 2020) and more recently (May 27, 2021) 18F-DCFPyL PET/CT was FDA approved, with immediate availability in parts of the mid-Atlantic and southern regions and more widespread availability throughout the United States by the end of 2021.
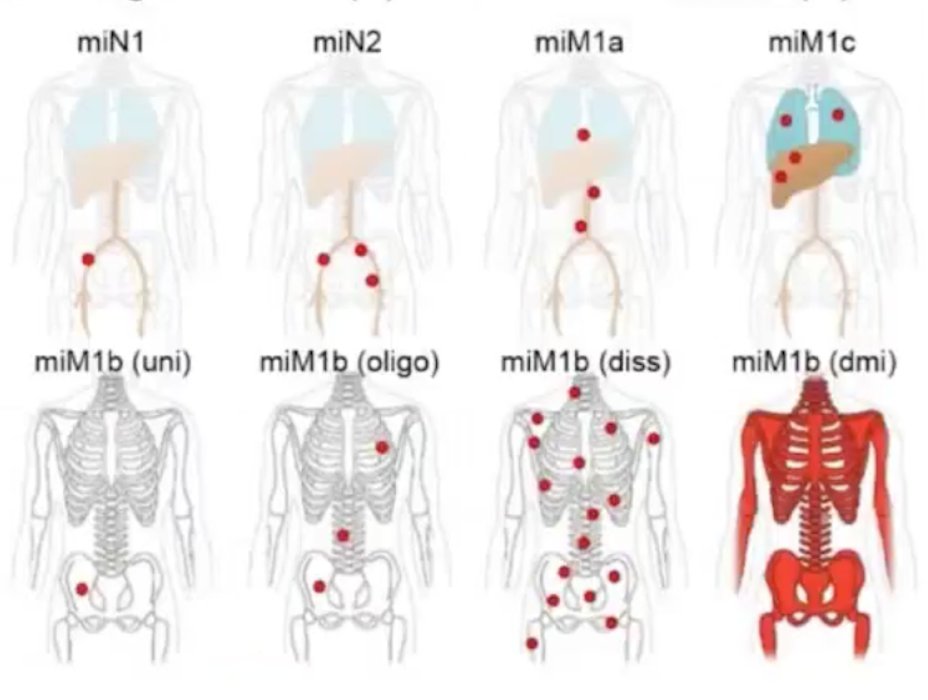
Dr. Calais emphasized the general rules for PET/CT (utilizing 9 different views + MIP), including commenting on lesion location, shape, size, multiplicity, homogeneous/heterogeneous characteristics, intensity, and lesions to background ratio. Ultimately, in concert with disease localization, clinicians need an estimate of the disease TNM classification:
Several trials have assessed the importance of PSA level with regards to detection rates. In 2019, the UCSF-UCLA prospective single-arm clinical trial of 68Ga-PSMA-11 was published.4 There were 635 men with biochemically recurrent prostate cancer after prostatectomy (n=262, 41%), radiation therapy (n=169, 27%), or both (n=204, 32%) that underwent 68Ga-PSMA-11 PET. PET/CT correctly localized lesions in 75% patients, with increased detection rates with increasing PSA: 38% for PSA <0.5 ng/mL, 57% for PSA 0.5 to < 1.0 ng/mL, 84% for PSA 1.0 to <2.0 ng/mL, 86% for PSA 2.0 to <5.0 ng/mL, and 97% for PSA >= 5.0 ng/mL:

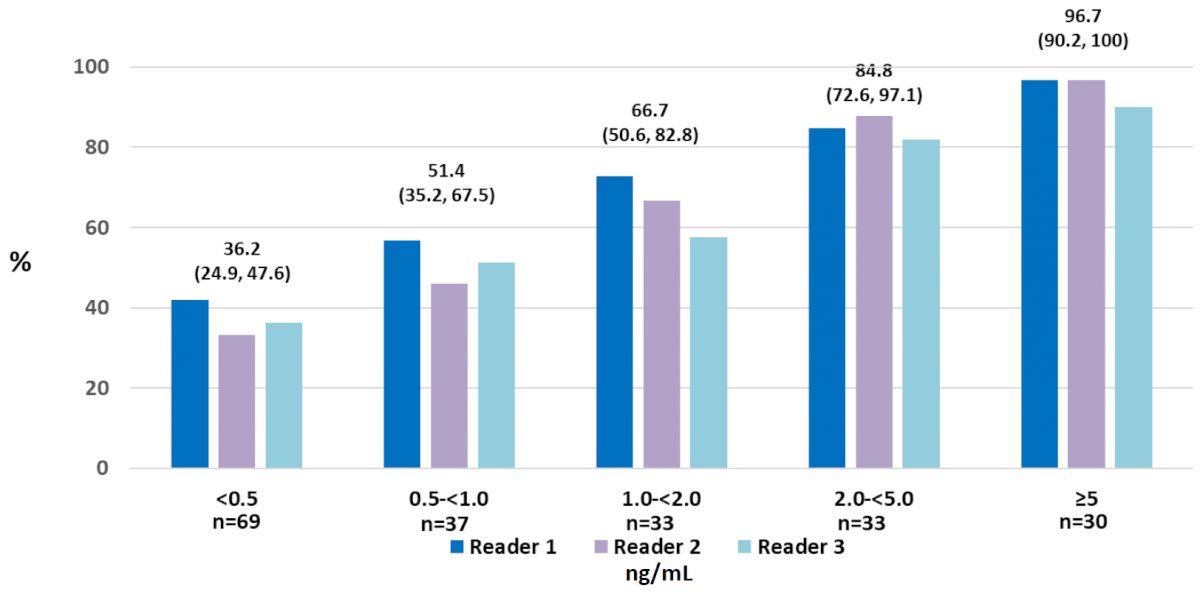
There were 208 patients in the CONDOR trial that underwent a DCFPyL-PET/CT, and those with a positive scan based on local interpretation were scheduled for follow up within 60 days to verify suspected lesion(s) using a composite standard of truth. The primary outcome of interest was the correct localization rate, defined as the percentage of patients with a 1:1 correspondence between at least one lesion identified by DCFPyL-PET/CT and the composite standard of truth: pathology, correlative imaging, or PSA response, in descending order of priority. Median PSA in this cohort was 0.8 [0.2 - 98.4] ng/mL. Using the defined primary outcome of correct localization rate, the authors demonstrated that DCFPyL-PET/CT correctly localized lesions in 84.8-87.0% of cases among the three readers (lower bound of 95% CI: 77.8%-80.4%), against the composite standard of truth. As follows is the detection rate by baseline PSA:
There are several pitfalls and challenges to PSMA PET/CT as highlighted by Dr. Calais including spondylophytes, avascular necrosis, hemangiomas (osseous venous vascular malformation), Paget Disease, severe osteonecrosis, bone trauma (particularly in the ribs), and degenerate cysts (lucent lesion with a sclerotic rim)
Dr. Calais concluded with the following summary messages:
- For indeterminate lesions, it is important to assess longitudinal temporal information, repeat scan(s), monitor the patient’s PSA, and follow-up in 3-6 months
- It is important to take into context the patient’s PSA and the clinical question of interest
- When first assessing a PSMA PET/CT, it is important to take a first look/global scenario view of the scan: MIP + WB PET coronal view
- The following characteristics are likely not associated with prostate cancer: faint, diffuse/not focal, isolated, symmetric, uncommon locations for prostate cancer spread, and CT correlative pattern
- The following characteristics are likely associated with being suspicious for prostate cancer: intense, focal, known other metastatic lesions, asymmetric, and common locations for prostate cancer spread
- From the clinician perspective, it is important to have high specificity (how do I treat these findings on imaging? Is this real?)
- From the PET physician's perspective, it is important to have high sensitivity (I must not miss this lesion!)
Presented by: Jeremie Calais, MD, MSc - Assistant Professor at the Ahmanson Translational Imaging Division of the Department of Molecular and Medical Pharmacology in the David Geffen School of Medicine at UCLA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the Society of Nuclear Medicine & Molecular Imaging – 2021 Virtual Meeting, June 11-15, 2021
References:
- Hofman MS, Lawrentschuk N, Francis, RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomized, multicentre study. Lancet 2020 Apr 11;395(10231):1208-1216.
- Calais J, Ceci F, Eiber M, et al. 18F-fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: A prospective, single-centre, single-arm, comparative trial. Lancet Oncol 2019 Sep;20(9):1286-1294.
- Harmon SA, Mena E, Shih JH, et al. A comparison of prostate cancer bone metastases on 18F-sodium fluoride and prostate specific antigen (18F-PSMA) PET/CT: Discordant uptake in the same lesion. Oncotarget. 2018 Dec 28;9(102):37676-37688.
- Fendler WP, Calais J, Eiber M, et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol. 2019 Jun 1;5(6):856-863.
- Morris MJ, Rowe SP, Gorin MA, et al. Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study. Clin Cancer Res. 2021 Feb 23 [Epub ahead of print].