This paved the way for robotic surgery because the sole purpose of the robotic platform is to make laparoscopic surgery easier for the surgeon. It is ergonomic, intuitive, it facilitates execution of surgical movements and it is associated with easier skill transfer. He then followed up by comparing 1800 RRP with 1537 LRP and the first 350 robot-assisted laparoscopic radical prostatectomies at the MSKCC with no differences in recurrence, urinary function recovery and sexual function recovery. The main criticism of the MSKCC trials was that the surgeries were performed in a single center by a few surgeons and the external validity of this data came into question. This issue was assessed by the Swedish LAPPRO study that included over 4000 patients and determined that robotic surgery had less blood loss, comparable readmission rates and reoperations with equivalent oncological and functional outcomes.
A phase 3 randomized clinical trial that included 326 patients comparing open RRP with robot-assisted LRP in Australia yielded similar functional and oncological outcomes at 24 months of follow up was recently published in Lancet Oncology. This provides level 1 evidence that proves no differences between both techniques.
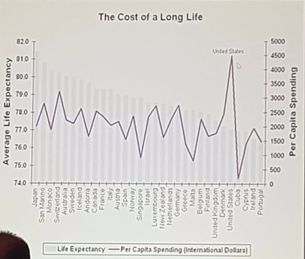
From a public health standpoint, robotic surgery implementation needs to be evaluated for its intrinsic value and determine if this technology is feasible for a health care system. Robot assisted LRP provides benefits for best patient outcomes (equivalent oncological outcomes with less pain and faster recovery) and helps standardize outcomes for surgeons. This taken into account, in a country such as Mexico, he cautioned that the ministry of health has to decide if this investment in technology is worthwhile for any given country. To conclude he states that buying more technology or increasing health care spending does not increase life expectancy (see Figure 1).
Presented by: Karim A. Touijer, MD, MPH from the Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Adrián M. Garza-Gangemi, MD, medical writer for UroToday.com and Ashish Kamat, MD, Professor of Urology and Director of Urologic Oncology Fellowship at M.D. Anderson Cancer Center, at the Mexican Urologic Oncology Association Meeting - July 26 - 28, 2018