The frequency of non-recognized histological subtypes by a community pathologist is an astonishing 44% of all the biopsy samples. This remark left a take-home message: Ask your pathologist if there is a histological subtype such as lymphoepithelial, plasmacytoid, nested variant, micropapillary and small cell histology.
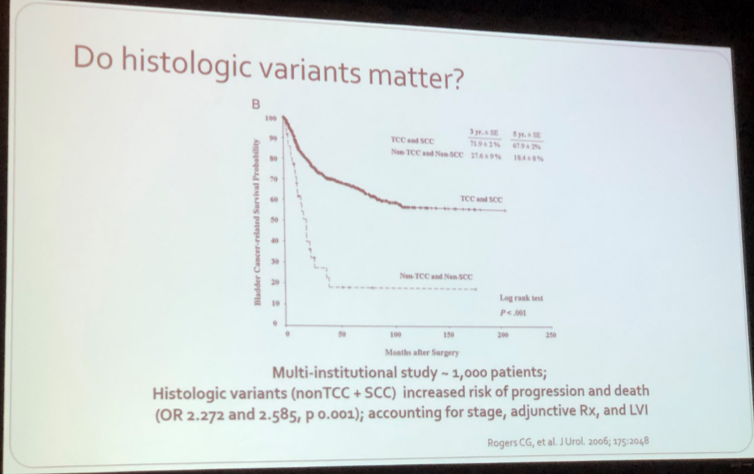
The later information takes importance when considering they have worst outcome regarding the higher propensity of locally advanced disease, greater degree of lymph node metastasis, an HR of 2.7 of upstaging at radical cystectomy and considering the different responses to therapy on this strains (Fig 1)
Figure 1:
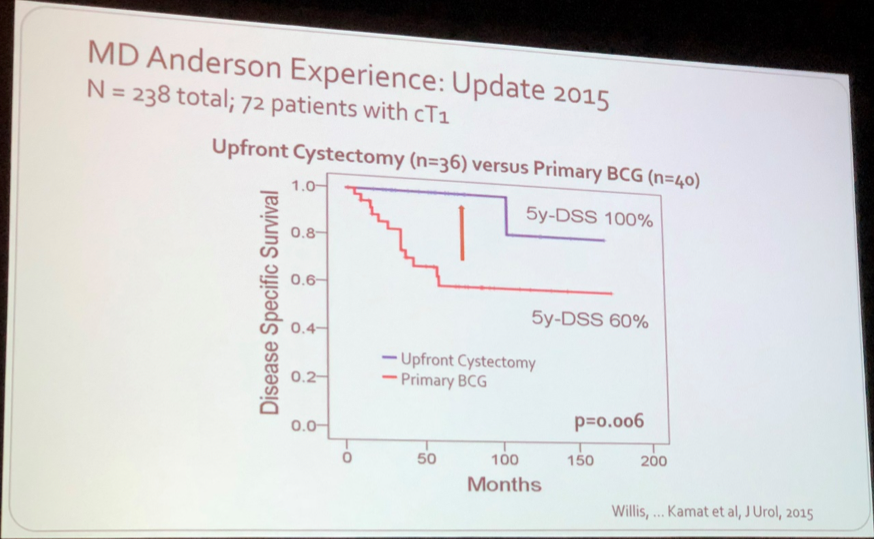
Micropapillary bladder cancer was first described at MD Anderson Cancer Center in 1994 as a rare subtype. It has two histological features that made this variant peculiar: the micropapillae without central vascular cores and the consisting lymphovascular invasion present in the micropapillary areas. Dr. Kamat showed evidence describing the poor performance of BCG in this variant, with 89% of recurrence and 67% of progression, 22% of them with metastasis (Fig 2), and the disease-specific survival (DSS) after progression is 24% at 5 years. Dr. Kamat dramatically depicted the chance of surviving micropapillary bladder cancer is lower than playing Russian roulette when treating MPBC with BCG only. The consensus of the best treatment for cT1MPBC was the radical cystectomy, and BCG only in very selected patients.
Figure 2:
The Small Cell Carcinoma differs biologically from urothelial carcinoma, for early metastasis, rapid growth and the unique metastasis sites (brain and bone). Approximately 50% of patients have metastasis at cystectomy, despite clinically organ-confined disease, thus, is considered initially as a systemic disease, and CNS image is mandatory for all patients. In this variant, the neoadyuvant chemotherapy (NAC) improves the overall survival (OS) (159.5 vs 18.3 months) and DSS at 5 years (79 vs 20%), the drugs of choice are cisplatin with etoposide, followed by radical cystectomy. For patients unable to undergo cystectomy, NAC followed by chemoradiotherapy is an alternative.
The squamous differentiation is found very common in urothelial cancer, found in up to 60%, often mixed with glandular differentiation. The biology of this tumor portends more aggressive behavior, nevertheless, has no impact in DSS, therefore it should be treated similarly as stage-matched urothelial bladder cancer, and NAC should be considered.
Dr. Kamat concluded his talk by stating the importance of awareness of bladder cancer variant histology and the impact in prognosis, and the treatment should be personalized by each patient
Speaker: Ashish M. Kamat, MD, Professor of Urologic Oncology, MD Anderson Cancer Center, Houston, TX
Written by: Ashmar Gómez Conzatti, MD, Urology Resident, Instituto Nacional de Ciencias Médicas y Nutrición “Salvador Zubirán”, Mexico City & Ashish M. Kamat, MD, Professor of Urologic Oncology, MD Anderson Cancer Center, Houston, TX at the 2018 Congreso de la Asociación Mexicana de Urología Oncológica – July 25-28, 2018, Acapulco, GRO México