(UroToday.com) The Société Internationale D’Urologie (SIU) 2021 annual meeting included a master class on advanced kidney cancer with a presentation by Dr. Ozcan Yildiz discussing new systemic therapies in advanced RCC. Dr. Yildiz started by highlighting that in 2000, the survival of metastatic RCC was quite poor, with a median OS of 5 months for those with poor-risk disease, 14 months for intermediate-risk disease, and 30 months for favorable-risk disease. Since then, there has been an explosion of FDA approvals for drugs in this disease space as highlighted in the following timeline:

Dr. Yildiz then discussed the CARMENA trial,1 which was a 450 patient trial of suitable candidates for nephrectomy that were randomly assigned, in a 1:1 ratio, to undergo nephrectomy and then receive sunitinib or to receive sunitinib alone. Randomization was stratified according to prognostic risk (intermediate or poor) in the MSKCC prognostic model, and the primary endpoint was overall survival. At the planned interim analysis, the median follow-up was 50.9 months, and the results in the sunitinib-alone group were non-inferior to those in the nephrectomy-sunitinib group with regard to overall survival (HR for death 0.89, 95% CI 0.71-1.10; upper boundary of the 95% CI for noninferiority, ≤1.20). The median overall survival was 18.4 months in the sunitinib-alone group and 13.9 months in the nephrectomy-sunitinib group:
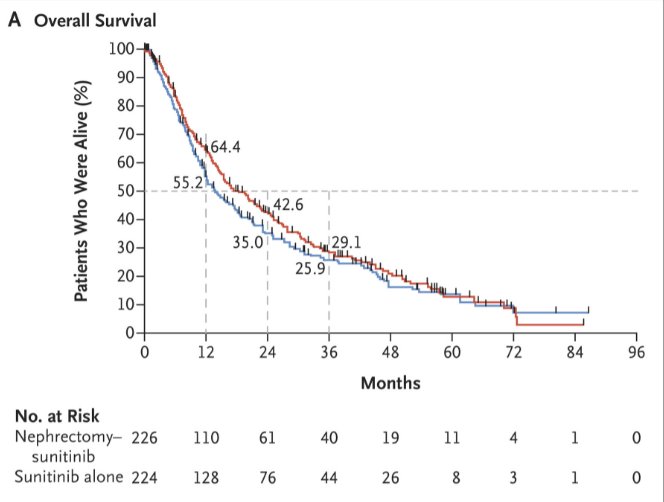
The investigators concluded that cytoreductive nephrectomy should no longer be part of standard of care for patients with metastatic RCC requiring medical treatment. Since CARMENA, the discussion has revolved around the importance of patient selection, specifically refraining from upfront cytoreductive nephrectomy in patients with liver metastases, T3-T4 tumors, low serum albumin, retroperitoneal supradiaphragmatic adenopathy, symptomatic bone or brain metastasis, and those with high LDH. Essentially, Dr. Yildiz notes that for any patient with 4 or more IMDC (Heng) criteria, nephrectomy is not beneficial.
When prioritizing agents for treating patients with metastatic RCC, there are several important aspects to consider, including prognostic classification, efficacy data, patient characteristics, comorbid illnesses, cost-effectiveness, quality of life, and patient preference. In a recent survey assessing patient preferences and expectations of systemic therapy, the question of “when thinking about therapy for your kidney cancer, based on your current situation, what is the most important desire or outcome do you want to see from treatment?” was posed to patients. The overwhelming majority of patients (>60%) stated that the chance of eliminating all evidence of disease (complete response) was their most important priority.
Currently, the approved first-line combination therapies in advanced RCC are as follows:

Dr. Yildiz then discussed several of the key phase 3 trials in more detail. In the CLEAR trial, patients with previously untreated advanced RCC were randomization in a 1:1:1 fashion to lenvatinib 20 mg orally once daily + pembrolizumab 200 mg IV every 3 weeks; or lenvatinib 18 mg + everolimus 5 mg orally once daily; or sunitinib 50 mg orally once daily (4 weeks on/2 weeks off in 6-weekly cycles).2 The authors assessed the primary endpoint of progression-free survival by Independent Review Committee per RECIST v1.1 with key secondary endpoints including OS, objective response rate (ORR), and safety. This trial randomized 1,069 patients, 355 who received lenvatinib and pembrolizumab, 357 who received lenvatinib and everolimus, and 357 who received sunitinib. Over a median follow-up of 27 months, PFS was significantly improved among patients receiving lenvatinib and pembrolizumab (median 24 months) vs sunitinib (median 9 months; HR 0.39, 95% CI 0.32–0.49) and among patients receiving lenvatinib and everolimus (median 15 months) vs sunitinib (HR 0.65, 95% CI 0.53–0.80).

The benefit of lenvatinib and pembrolizumab versus sunitinib with respect to progression-free survival was consistent across many subgroups, comprising age, sex, geographic region, PD-L1 expression, IMDC risk group, prior nephrectomy, and sarcomatoid features. Further, OS was significantly longer among patients who received lenvatinib and pembrolizumab compared to sunitinib (HR 0.66, 95% CI 0.49–0.88), whereas there was no significant difference in OS for patients receiving lenvatinib and everolimus compared to sunitinib (HR 1.15, 95% CI 0.88–1.50):

As with progression-free survival, these findings were consistent across all relevant tested subgroups for the comparison of lenvatinib and pembrolizumab, except patients with favorable-risk group. Grade ≥3 treatment-related adverse events occurred in 72% of patients in the lenvatinib and pembrolizumab arm and 73% of patients in the lenvatinib and everolimus arm compared with 59% of patients in the sunitinib arm. Based on the results of the CLEAR trial, on August 10, 2021, the FDA approved lenvatinib plus pembrolizumab for first-line treatment of advanced RCC.
In KEYNOTE-426, 861 patients with metastatic clear cell RCC, predominately with intermediate or poor-risk disease, who had not previously received systemic therapy were randomized to pembrolizumab + axitinib or sunitinib and followed for the co-primary endpoints of overall survival and progression-free survival.3 While median OS was not reached, patients who received pembrolizumab + axitinib had improved OS (HR 0.53, 95% CI 0.38 to 0.74) and progression-free survival (HR 0.69, 95% CI 0.57 to 0.84), as well as overall response rate. These results were consistent across subgroups of demographic characteristics, IMDC risk categories, and PD-L1 expression level. With a median follow-up of 30.6 months, clinically meaningful responses were sustained, including a median overall survival of not reached versus 35.7 months favoring pembrolizumab + axitinib (HR 0.68, 95% CI 0.55-0.85).4 The most recent updated follow-up of this trial (median 42.8 months) was presented at ASCO 2021, showing a durable survival benefit for pembrolizumab + axitinib (HR 0.73, 95% CI 0.60-0.88):

In the CheckMate 9ER trial, 651 patients were randomized in a 1:1 fashion to nivolumab + cabozantinib or sunitinib, in the first-line treatment of patients with advanced or metastatic renal cell carcinoma, with randomization was stratified by IMDC risk score, tumor PD-L1 expression, and region.5 The primary outcome was progression-free survival with overall survival, objective response rate, and toxicity comprising important secondary outcomes. Over a median follow-up of 18 months, median progression-free survival was significantly longer among those randomized to nivolumab + cabozantinib (16.6 months) than those randomized to sunitinib (8.3 months), with a relative difference of 49% (HR 0.51, 95% CI 0.41 to 0.64):
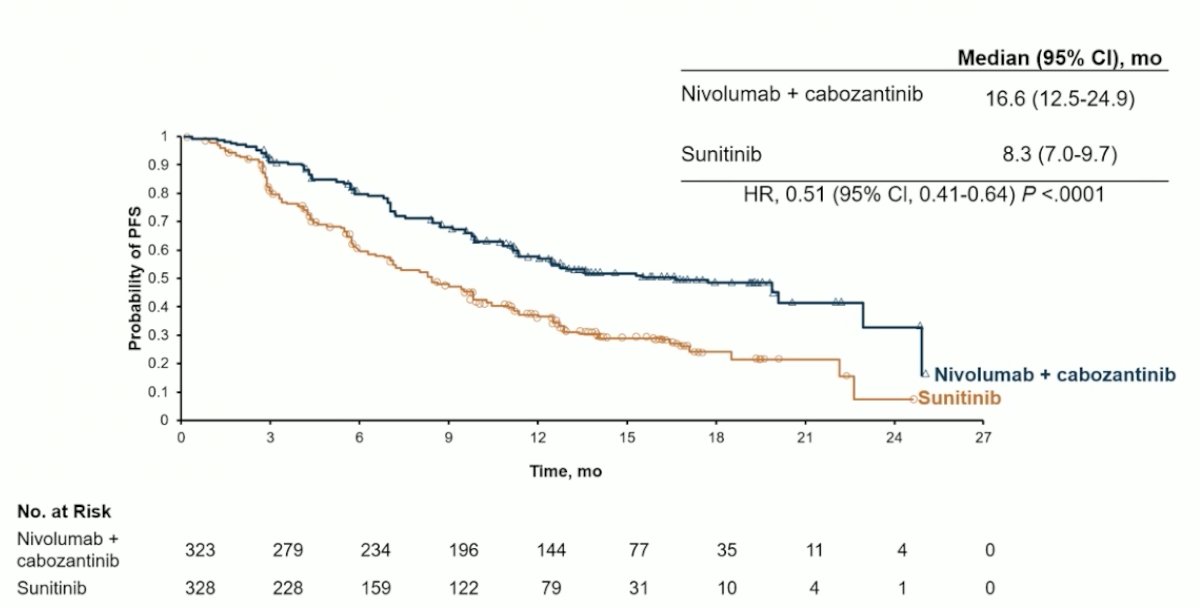
OS was not reached in either arm (HR 0.60, 98.89% CI 0.40 to 0.89). Notably, these benefits were seen consistently across pre-specified subgroups defined according to IMDC risk categories and PD-L1 expression. Any grade treatment-related adverse events were common in both groups: 96.6% among those receiving nivolumab + cabozantinib and 93.1% among those receiving sunitinib. High-grade events (grade 3 or greater) were somewhat higher among those receiving nivolumab + cabozantinib (60.6% vs 50.9%). One grade 5 event occurred in the nivolumab + cabozantinib arm while 2 occurred in the sunitinib treated group. Importantly, quality of life was maintained for those receiving nivolumab + cabozantinib while there was a decline in quality of life among those receiving sunitinib. On January 22, 2021, the FDA approved nivolumab plus cabozantinib for first-line treatment of advanced RCC. In a subsequent update with a data cutoff of September 10, 2020, PFS continues to remain stable (HR 0.52, 95% CI 0.43-0.64), with OS still not reached (HR 0.66, 95%CI 0.50-0.87).
The CheckMate 214 trial tested nivolumab + ipilimumab in newly diagnosed clear-cell RCC; the trial schema for CheckMate 214 is as follows:6

Now with a minimum of 60 months of follow-up data first presented at ESMO 2021, the combination of nivolumab + ipilimumab has shown a durable PFS and OS benefit (HR 0.68, 95% CI 0.58-0.81) among intermediate/poor-risk patients:

Dr. Yildiz then discussed a representative case of a 41-year-old female patient that was seen in April 2020 secondary to gross hematuria and left flank pain. A CT demonstrated an 8-cm enhancing mass in the left kidney and a 3 cm lesion in the right sacroiliac joint. The patient was scheduled to have a biopsy, but this was delayed secondary to her having COVID-19, and the patient was lost to follow-up until November 2020. At this point, an MRI showed that the mass was now 9.4 cm in the kidney and the lesion in the sacroiliac joint was now 5 cm. A bone biopsy demonstrated clear cell RCC, hemoglobin was 9.7, and ECOG performance status was 1. The patient received SBRT to the bone lesion and was started on nivolumab + ipilimumab + zoledronic acid, with a partial response in the kidney primary and complete response of the osseous metastasis.
With regards to cytoreductive nephrectomy in patients treated with targeted therapy or immune checkpoint inhibitors, previous work presented at the 2020 GU ASCO meeting showed cytoreductive nephrectomy was associated with improved overall survival in patients treated with either first-line targeted therapy (HR 0.48, 95% CI 0.45-0.52) or first-line immune checkpoint inhibitors (HR 0.44, 95% CI 0.30-0.64):

There are several trials currently enrolling patients in the context of cytoreductive nephrectomy in the immunotherapy era, including the NORDIC-SUN trial which is an open-label phase 3 randomized trial of deferred cytoreductive nephrectomy in synchronous metastatic RCC receiving checkpoint inhibitors. Approximately 400 patients will be randomized to surgery after induction therapy (nivolumab + ipilimumab) followed by maintenance nivolumab versus induction therapy (nivolumab + ipilimumab) followed by maintenance nivolumab (no surgery). The primary outcome for this trial is overall survival over a minimum of three years of follow-up.
The aforementioned patient subsequently underwent a cytoreductive nephrectomy, showing complete necrosis in the tumor (complete response). In the patient preferences survey regarding expectations of systemic therapy, another question included “Current treatments for RCC require continuous therapy. However, research suggests that patients might be able to discontinue therapy after a period of time and maintain efficacy. If your doctor suggested stopping your therapy because your disease was well controlled, how would you feel?” 58% of patients said they would be anxious about their cancer progression, 20% would want to stay on therapy, and 12% said they would feel safer being able to avoid future side effects of treatment. There are many options in the front-line setting and many considerations and opportunities for shared decision making, as highlighted in the following table:

Dr. Yildiz concluded his presentation of new systemic therapies in advanced RCC with the following take-home messages:
- Frontline management of metastatic RCC has been transformed in recent years
- IO/TKI regimens lead to the highest ORR/longest PFS and are useful for early disease and symptom control
- Dual IO has the potential advantages in the duration of disease control
- Patients are anxious about disease control and may overlook concerns related to toxicities that could result in severe adverse events
- Communicating the risk/benefit ratio to patients is important when discussing treatment options
- Encouraging patients to openly communicate about adverse events early when starting therapy is crucial
Presented by: Ozcan Yildiz, MD, Department of Medical Oncology, Istanbul Medipol University, Istanbul, Turkey
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 Société Internationale D’Urologie (SIU) Hybrid Annual Meeting, Wed, Nov 10 – Sun, Nov 14, 2021.
References:
- Mejean A, Ravaud A, Thezenas S, et al. Sunitinib alone or after nephrectomy in metastatic renal cell carcinoma. N Engl J Med 2018 Aug 2;379(5):417-427.
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. 2021 Apr 8;384(14):1289-1300.
- Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med 2019;380(12):1116-1127.
- Powles T, Plimack ER, Soulieres D, et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomized, open-label, phase 3 trial. Lancet Oncol. 2020 Dec;21(12):1563-1573.
- Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021 Mar 4;384(9):829-841.
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carinoma. N Engl J Med 2018;378(14):1277-1290.