Dr. Briganti notes that extended pelvic lymph node dissection provides important information for staging and prognosis, which cannot be matched by any other currently available procedure. A risk of nodal metastases over 5% (as calculated by the Briganti nomogram or Roach formula) is an indication to perform an extended pelvic lymph node dissection, with a strength rating of strong by the EAU guidelines on prostate cancer. Among 497 patients diagnosed via MRI-targeted biopsies and treated with radical prostatectomy and extended pelvic lymph node dissection, Gandaglia et al. found that a model including prostate-specific antigen (PSA), clinical stage and the maximum diameter of the index lesion on multiparametric MRI, grade group on targeted biopsy, and the presence of clinically significant prostate cancer on concomitant systematic biopsy had an area under the curve (AUC) of 86% and represented the basis for a coefficient-based nomogram.1 Using a cutoff of 7%, 244 extended pelvic lymph node dissection (57%) would be spared and a lower number of lymph node invasions (LNI) (1.6%) would be missed compared to other available nomograms.
Dr. Briganti notes that the optimal extent of a pelvic lymph node dissection includes extending the dissection along common iliac vessels at least up to the ureteric crossing. With this approach, 75% of all lymph nodes potentially harboring lymph node invasion can be removed:2
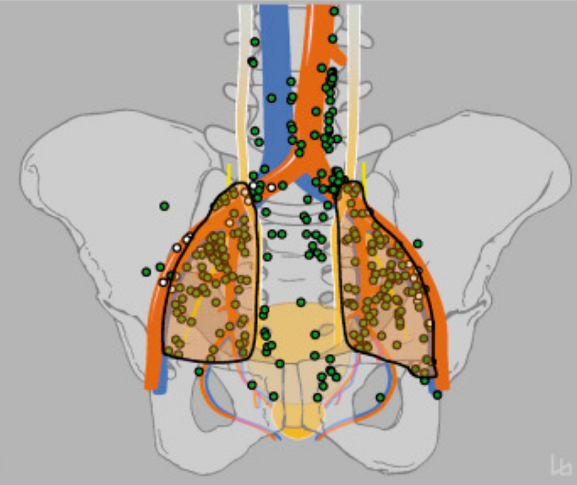
Dr. Briganti notes that there may be a subset of patients that may also benefit from staging from a super-extended pelvic lymph node dissection. Among 471 patients with high-risk prostate cancer treated with radical prostatectomy (RP) and a super-extended pelvic lymph node dissection (PLND) that included the removal of the pre-sacral and common iliac nodes, the median preoperative LNI risk was 25.5% with a median number of nodes removed of 23 – lymph node invasion was noted in 36.3% of patients.3 The adoption of a 30% threshold would result in avoiding the removal of the common iliac and pre-sacral nodes in >60% cases, with a risk of missing LNI in these regions of <5%. However, there is no data on the impact of such an extensive approach on cancer control.
The main pros of pelvic lymph node dissection are as follows:
- Optimal staging
- Identification of candidates for adjuvant therapies
- Possibly, improved oncologic control
Dr. Briganti suggests that we may be tempted to replace lymph node staging with prostate-specific membrane antigen (PSMA) PET-CT for nodal staging. However, he cautions that the sensitivity per lymph node for PSMA PET-CT typically is ~60%. The reason for this is that these patients may have micrometastatic disease. For patients with <2 mm diameter lymph node metastasis, the detection of PSMA is 0%, with a prevalence at extended pelvic lymph node dissection of 20%. For >5 mm diameter lymph node metastasis, the detection of PSMA is 86%, with a prevalence at extended pelvic lymph node dissection of 40%.
Given that the benefit of pelvic lymph node dissection is still unknown with regards to cancer control, randomized controlled trials are desperately needed. As follows is a list of ongoing clinical trials in this disease space, specifically extended lymph node dissection versus limited or no pelvic lymph node dissection:
According to Dr. Briganti, the following are cons with regards to pelvic lymph node dissection for prostate cancer:
- Longer operative time and complications
- Many unnecessary pelvic lymph node dissections are still performed (while waiting for the results from randomized controlled trials)
Data from a meta-analysis in press at European Urology Oncology assessing 176 studies suggest that the impact of extended pelvic lymph node dissection on peri-operative morbidity includes vascular injuries (0.4%), nerve injuries (1%), and lymphocele formation (extended pelvic lymph node dissection was confirmed as an independent predictor, RR 1.77). Data presented at the 2017 American Society of Clinical Oncology (ASCO) meeting from Brazil also shows the following complications comparing extend versus limited pelvic lymph node dissection: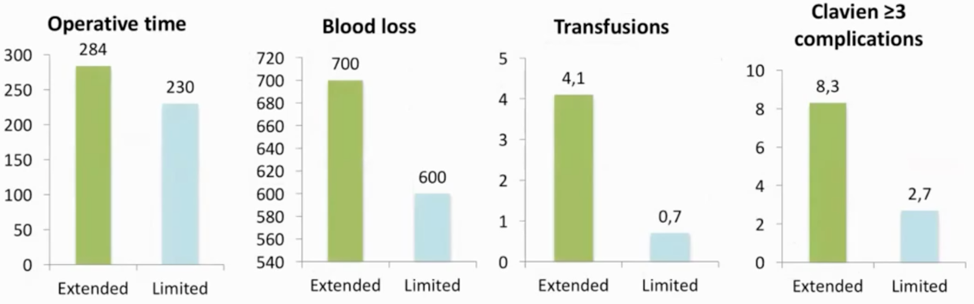
Dr. Briganti concluded with the following take-home messages from his talk on lymphadenectomy in prostate cancer:
- Extended pelvic lymph node dissection is the most accurate staging procedure for nodal staging
- Imaging cannot yet replace the need for an extended pelvic lymph node dissection
- Extended pelvic lymph node dissection includes removal of the obturator, external iliac, and hypogastric lymph nodes +/- pre-sacral and common iliac nodes
- The pros: timely delivery of post-operative treatments, and possibly cancer control in select men
- The cons: higher risk of intraoperative and perioperative complications
Presented by: Alberto Briganti, MD, PhD, Associate Professor of Urology, Università Vita-Salute San Raffaele, Deputy Director of Urological Research Institute (URI), IRCCS San Raffaele Scientific Institute, Milan, Italy
Written by: Zachary Klaassen, MD, MSc, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Augusta, Georgia, Twitter: @zklaassen_md at the 2020 Société Internationale d'Urologie Virtual Congress (#SIU2020), October 10th - October 11th, 2020
References:
1. Gandaglia, Giorgio, Guillaume Ploussard, Massimo Valerio, Agostino Mattei, Cristian Fiori, Nicola Fossati, Armando Stabile et al. "A novel nomogram to identify candidates for extended pelvic lymph node dissection among patients with clinically localized prostate cancer diagnosed with magnetic resonance imaging-targeted and systematic biopsies." European urology 75, no. 3 (2019): 506-514.
2. Mattei, Agostino, Frank G. Fuechsel, Nivedita Bhatta Dhar, Sebastian H. Warncke, George N. Thalmann, Thomas Krause, and Urs E. Studer. "The template of the primary lymphatic landing sites of the prostate should be revisited: results of a multimodality mapping study." European urology 53, no. 1 (2008): 118-125.
3. Gandaglia, Giorgio, Emanuele Zaffuto, Nicola Fossati, Marco Bandini, Nazareno Suardi, Elio Mazzone, Paolo Dell'Oglio et al. "Identifying candidates for super‐extended staging pelvic lymph node dissection among patients with high‐risk prostate cancer." BJU international 121, no. 3 (2018): 421-427.