To begin, he gave an overview of cancer treatments in 2020 emphasizing that for localized solid cancers, surgery or radiotherapy may be curative; for metastatic cancers, systemic therapy remains rarely curative; and for locally advanced cancers, surgery may be combined with systemic therapy to improve outcomes. To better examine its central role in many cancer treatments, it is worthwhile to consider how cancer surgery works. In many ways, the answer to this is unclear, likely much of carcinogenesis and cancer progression.
While certain steps in the metastatic disease progression have been characterized, the overall process is poorly understood. However, it is clear that not all cancers are equal in terms of their ability to progress and metastasize. Early-stage and low-grade cancers generally have not developed the ability to invade beyond the primary site. As a result, less aggressive therapy may be sufficient.
However, at the other end of the spectrum is locally advanced and limited metastatic disease. It is fairly well established that circulating tumor cells (CTC) or tumor DNA are present in patients with nearly all cancers. Given that surgery cannot remove these circulating tumor cells, how can we explain when surgery is curative in these individuals? Either the CTCs detected lack the ability to develop into secondary tumors, or the immune system destroys these cells before they are able to do so.
He then used the example of renal cell carcinoma with venous thrombus. Despite the fact that these tumors have already invaded into the largest vessels in the body, nearly half of patients without metastases at the time of surgery do not subsequently develop metastases following surgery. Thus, these tumors have developed the ability to intravasate into vessels but not the ability to adhere, extravasate, and form secondary tumors.
Considering testis cancer, these patients remain curable in the face of metastatic disease, unlike many other solid tumors, with multi-modality therapy. And, in spite of the chemotherapeutic sensitivity of these tumors, there remains an active role of surgical resection both of the primary tumor and metastatic nodal disease. Emphasizing data going back to 1959, Dr. Abel highlighted that nearly half of patients with micro-metastatic disease could be cured with retroperitoneal lymph node dissection.
Considering again renal cell carcinoma, for patients with nodal involvement with tumor, there remains a non-zero (and likely ~15%) chance of radiographic progression-free survival following surgical extirpation. Dr. Abel postulated that, for those patients, the immune system is likely responsible for destroying residual micro-metastatic disease.
In this context, Dr. Abel provided a brief review of how the immune system interacts with cancer cells, highlighting the role of cellular immunity with T-cells recognizing abnormal peptides, clonal expansion, targeting to the site of disease, and cancer cell killing.
Somewhat simplistically, Dr. Abel suggested that we may envision the benefit of surgery in patients with advanced cancer as a debulking such that the immune system has many fewer cancer cells to kill. However, the reality is likely much more complex than that.
Dr. Abel then highlighted that it has been long recognized that renal cell carcinoma is an immunologically active tumor. Beginning with cytokine based approaches and now transitioning to immune checkpoint modulators, therapies targeting the immune system have demonstrated benefit in this disease. Recently, data using combinations of inhibition of CTLA-4 and PD-1 or VEGF and PD-1 have demonstrated significant benefits in patients with advanced renal cell carcinoma based on data from CheckMate214, KEYNOTE-426, JAVELIN Renal 100, and CheckMate-9ER. These approaches have now become the standard of care.
Dr. Abel suggested that potentially more impressive than the improvements in overall and progression-free survival were the rates of complete response. In CheckMate214 this was 9% (compared with 1% among controls) and in KEYNOTE-426 this was 6% (compared with 2% in controls).
Notably, these agents have been investigated primarily among individuals who have already received nephrectomy, with rates ranging from 80% to 96%.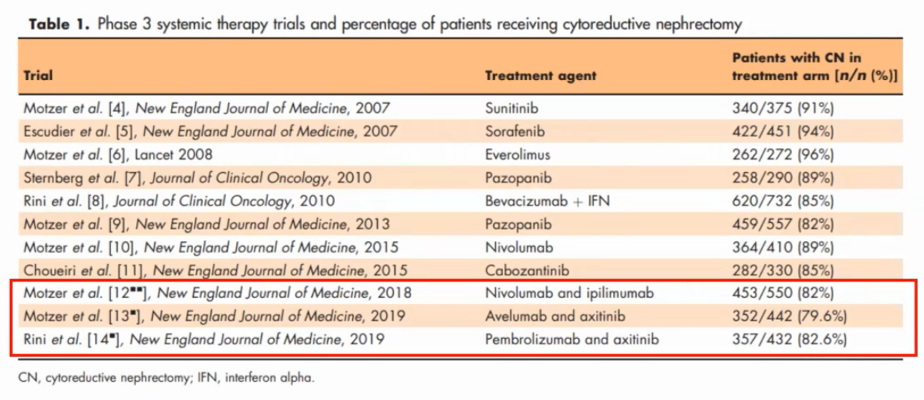
Thus, taken most explicitly, Dr. Abel argued that there is relatively little data to use these systemic therapy approaches in patients who have not undergone surgical resection.
Dr. Abel then highlighted the role of cytoreductive nephrectomy, beginning with the SWOG 8949 and EORTC30947 trials in the cytokine era which demonstrated improved median overall survival (pooled ~5-6 month advantage) with the conclusion that surgery likely benefits some patients though these were difficult the define. However, surgery did not make interferon work better and the mechanism of benefit is unclear.
Dr. Abel then discussed the CARMENA trial aimed at assessing the role of nephrectomy among patients receiving sunitinib for metastatic renal cell carcinoma. He emphasized that the trial closed due to poor enrollment in spite of an interim analysis failing to reach an endpoint for early closing. Also notable is that during the period of enrollment, checkpoint inhibitors had become standard of care for patients with poor-risk disease, who represented a large proportion of the study cohort.
While analysis was correctly performed on an intention to treat basis, Dr. Abel highlighted that actual treatment received varied quite substantially this nearly 20% of patients randomized to sunitinib alone receiving nephrectomy and 17% of those randomized to surgery and sunitinib never receiving sunitinib.
In spite of this, we may conclude that sunitinib alone is non-inferior among patients with a high metastatic burden though overall survival is lower than anticipated due to an enrichment of high-risk patients.
Given the data from CARMENA, for urologists considering cytoreductive nephrectomy, patient selection is critical and should generally reserve this approach for patients with good performance status, favorable or intermediate-risk disease, and symptomatic primary tumors.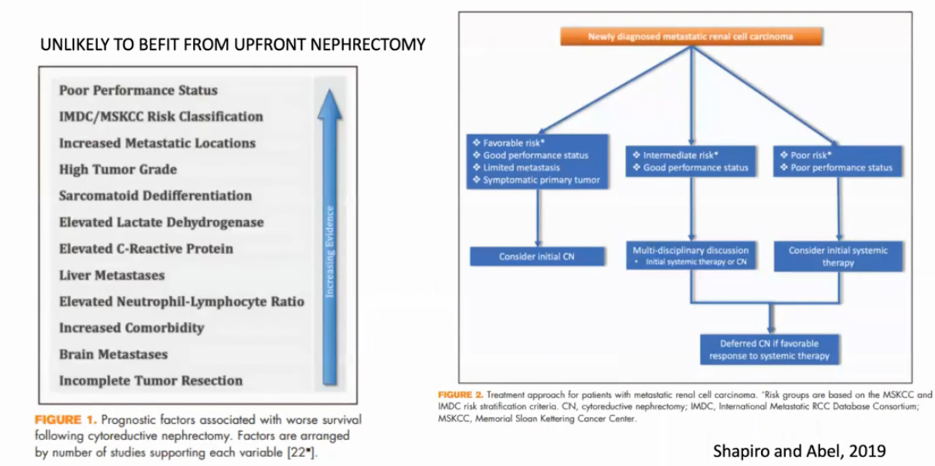
Currently, there are no direct data for the role of cytoreduction in patients receiving immune checkpoint inhibitors. Dr. Abel feels that surgical resection (both cytoreductive nephrectomy and metastasectomy) will remain a part of the multimodality treatment of locally advanced and metastatic cancer.
Presented by: E. Jason Abel, MD, FACS, Faculty, Department of Urology, University of Wisconsin School of Medicine and Public Health, University of Wisconsin, Madison, Wisconsin
Written by: Christopher J.D. Wallis, MD, PhD, Urologic Oncology Fellow, Vanderbilt University Medical Center, Nashville, Tennessee, Twitter: @WallisCJD at the 2020 Société Internationale d'Urologie Virtual Congress (#SIU2020), October 10th - October 11th, 2020