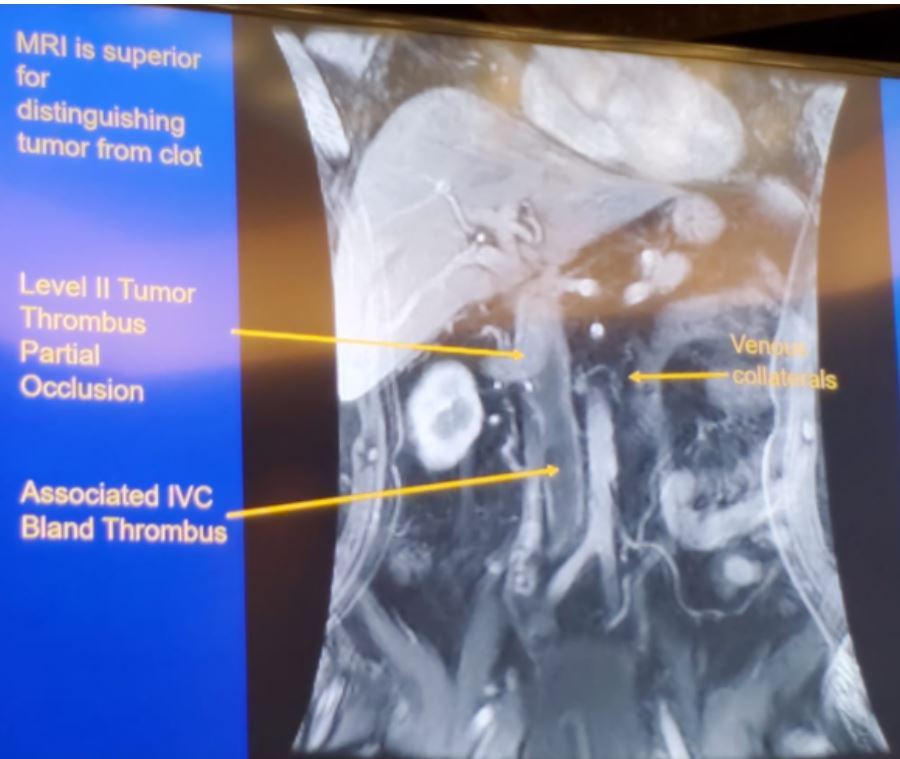
According to Dr. Leibovitch, the best imaging modality to use in these cases is MRI. MRI is superior for distinguishing tumor from a clot, as can be seen in Figure 1. The thrombus can progress rapidly and therefore performing an updated imaging scan (one week before surgery) is mandated. It is also important to consider anticoagulation when the IVC is severely occluded or nearly occluded, and when there is a bland thrombus. There is no need to place an IVC filter preoperatively. Lastly, staging as for any other advanced renal mass should be performed.
Figure 1 – MRI for distinguishing tumor thrombus and bland thrombus:
Data on patients with VTT who were not managed surgically showed poor prognosis.
Candidates for non-operative management include:
- Patients with poor performance status
- Acute/fulminant Budd-Chiari
- Bulk/critical metastatic disease
Dr. Leibovitch continued to describe his surgical principles for tumor thrombectomy:
- Assemble an experienced team – urologist, vascular, anesthesia, hepatobiliary surgeon, and cardiac surgeon if needed
- Operate on vessels first
- Ligate the renal artery, no need to embolize
- Isolate venous structures, consider the venous return
- Completely remove thrombus
- Mange any distal bland thrombus
- Repair/patch/replace IVC as needed
The incision itself should provide maximum exposure, whether it is done with a midline incision, bilateral subcostal (Chevron), or thoracoabdominal.
The volume of surgeries is important and impacts outcomes. In a large Canadian study assessing 816 cases between 1998 and 2007, the in-hospital mortality was 7.2%, with 75% of deaths occurring in the first 2 cases a surgeon performed.1 Increased surgeon volume was shown to be associated with lower in-hospital mortality.
Dr. Leibovitch believes that there is no need for preoperative embolization. There is data showing that embolization actually increased blood loss, complications, and mortality.2 Another important surgical tip is to pay attention to altered venous anatomy (Figure 2).
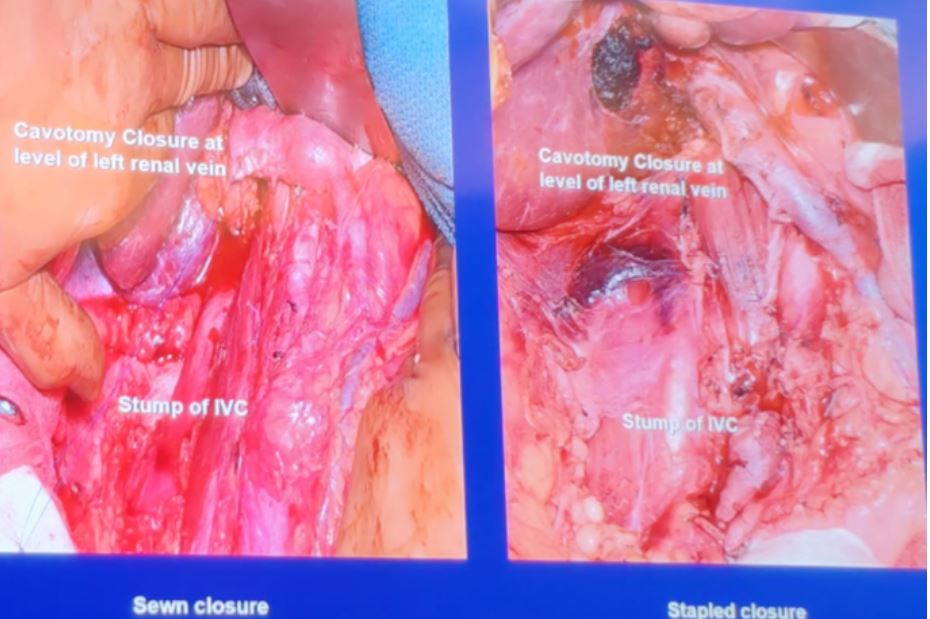
Next, Dr. Leibovitch showed how to manage a bland thrombus in the IVC or iliac veins (Figure 3). If the IVC needs to be resected due to complete occlusion caused by a bland thrombus, the cavotomy closure can be done as sewn or stapled closure (Figure 4).
Figure 2 – Altered venous anatomy:
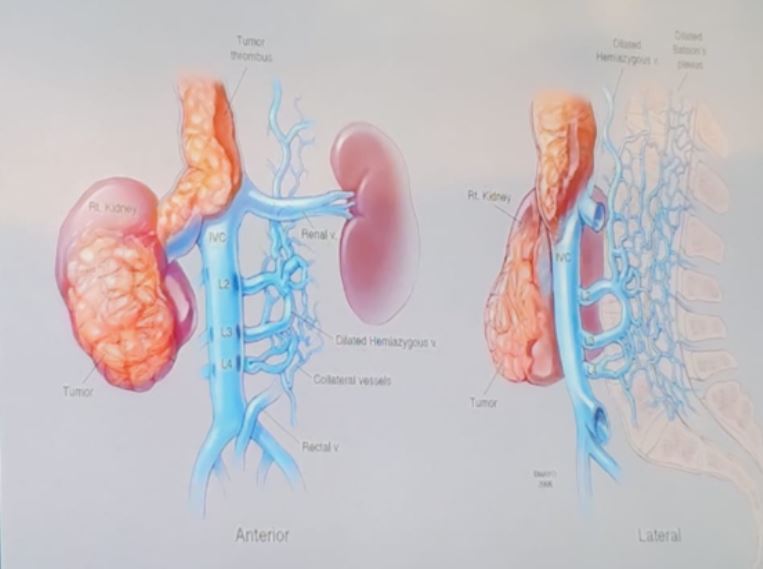
Figure 3 – How to manage a bland thrombus:
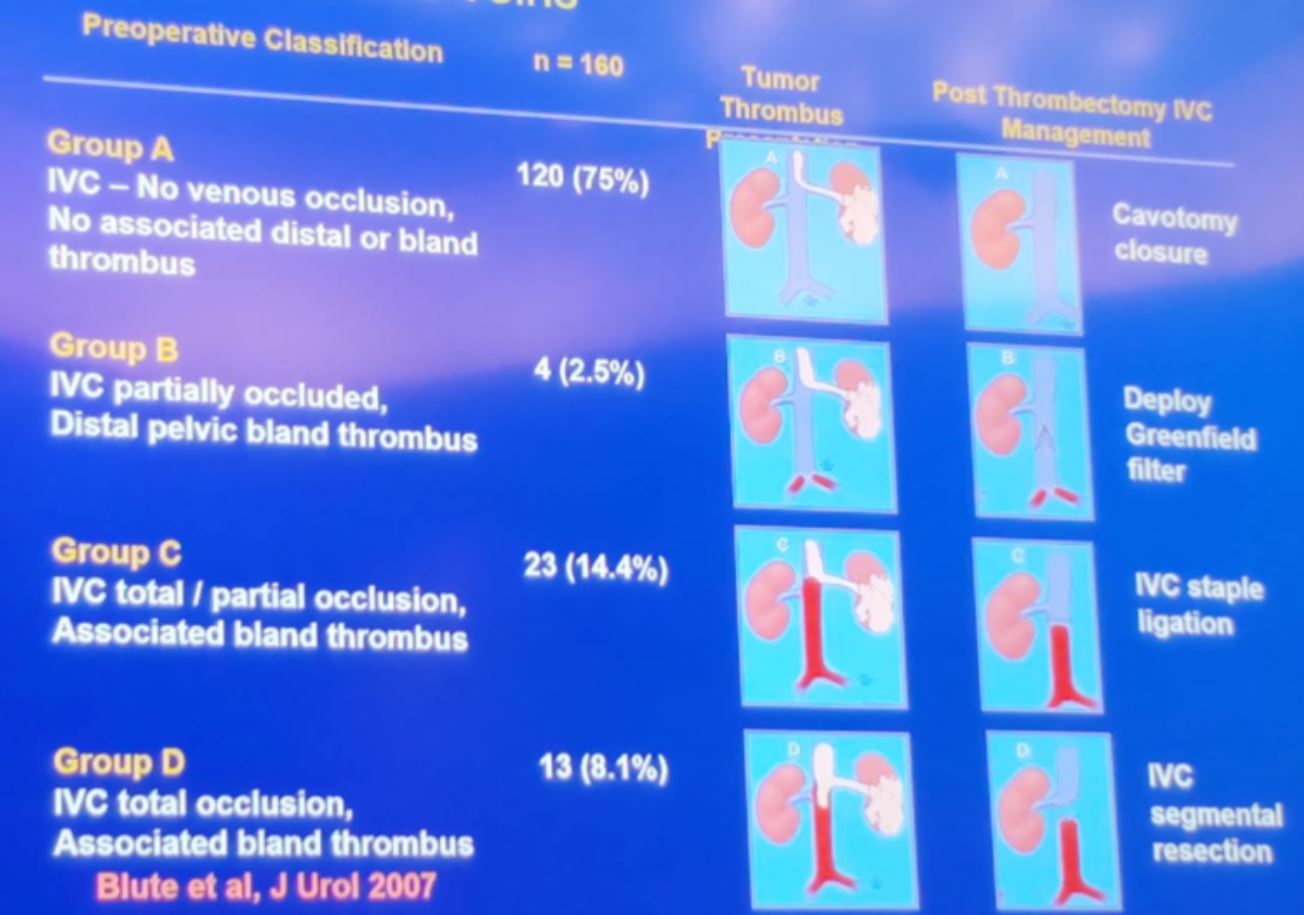
Figure 4 – Cavotomy closure techniques following IVC ligation:
The techniques for the surgical treatment of VTT at each level were described next. For level 1 or 2:
- Occlude renal artery first
- Ligate hepatic veins from the caudate lobe of the liver
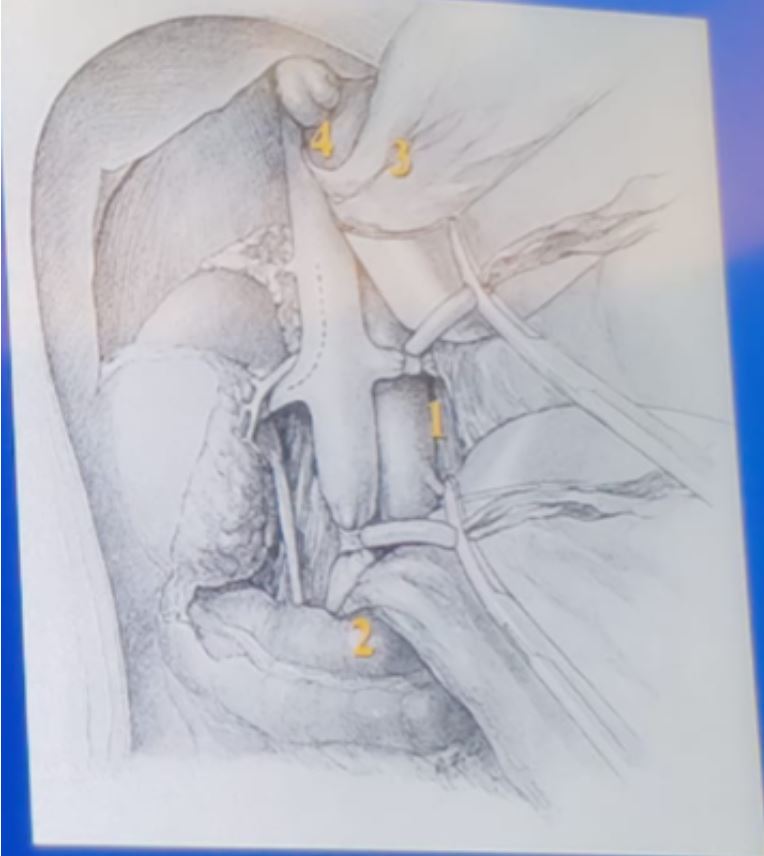
- Simple occluding maneuvers (contralateral renal vein, IVC inferior and superior to the VTT) (Figure 5)

For level 3 tumor thrombus (Figure 6):
- Renal artery ligation
- Mobilize liver for supra-hepatic IVC access
- Sequence for venous control:
- Contralateral renal vein
- Distal IVC
- Hepatic inflow (pringle maneuver)
- Supra-hepatic IVC (above thrombus)
- Remove thrombus
- Occlude IVC below the hepatic inflow
- Release supra-hepatic IVC and pringle
- Repair Vena cava leisurely
For tumor thrombus level 4:
- Requires constant hemodynamic monitoring
- Monitor thrombus in the atrium and / or IVC
- Assess the adequacy of resection
- Use veno-veno bypass or cardiopulmonary bypass +/- hypothermic (16 degrees Celsius) circulatory arrest
Figure 7 - Cancer-specific survival by stage:

Dr. Leibovitch concluded his talk mentioning several future directions. These include the role of neoadjuvant therapy and minimally invasive surgery, which will be further explored.
Presented by: Bradley Leibovich, MD, Department of Urology, Mayo Clinic, Rochester, Minnesota
Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, New York, USA, Twitter: @GoldbergHanan at the 39th Congress of the Société Internationale d'Urologie, SIU 2019, #SIUWorld #SIU2019, October 17-20, 2019, Athens, Greece
References:
1. Toren P, Abouassaly R, Timilshina N, Kulkarni G, Alibhai S, Finelli A. Results of a national population-based study of outcomes of surgery for renal tumors associated with inferior vena cava thrombus. Urology 2013; 82(3): 572-7.
2. Subramanian VS, Stephenson AJ, Goldfarb DA, Fergany AF, Novick AC, Krishnamurthi V. Utility of preoperative renal artery embolization for management of renal tumors with inferior vena caval thrombi. Urology 2009; 74(1): 154-9.
3. Psutka SP, Leibovich BC. Management of inferior vena cava tumor thrombus in locally advanced renal cell carcinoma. Ther Adv Urol 2015; 7(4): 216-29.
4. Blute ML, Leibovich BC, Lohse CM, Cheville JC, Zincke H. The Mayo Clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus. BJU international 2004; 94(1): 33-41.