In the prospective PAIREDCAP trial1, 226 biopsy naïve men with an elevated PSA underwent an mpMRI. They were divided to whether a PIRADS lesion 3 or above was found, to those who were found with a PIRADS lesion less than 3. Those with PIRADS<3 underwent a systematic biopsy (n=50) with clinically significant prostate cancer being diagnosed in 16% of cases. In contrast, those with PIRADS >=3 lesion underwent a systematic biopsy, a cognitive targeted biopsy and an mpMRI-US fusion targeted biopsy (n=176). This arm had clinically significant prostate cancer diagnosed in 69% of cases. Targeted biopsy provided only marginal benefit over standard biopsy to detect clinically significant prostate cancer in biopsy nave men with PIRADS >=3. However, the combination of both targeted biopsy and systematic biopsy lead to the highest detection rate.
When assessing the role of mpMRI prior to confirmatory biopsy in patients being treated with active surveillance, all grade reclassification to Gleason 4+3 or higher was in men with PIRADS 4 or 5. 2
Summing up these data, mpMRI may still miss some of the clinically significant prostate cancer with targeted biopsy alone, and therefore combining it with systematic biopsy is advisable. It also has an important role in grade reclassification in active surveillance.
Dr. Tilki moved on to discuss the role of mpMRI and biomarkers in daily practice. The first setting discussed was patient selection for re-biopsy. The relevant biomarker is ConfirmMDx. This test detects a field effect or halo associated with the presence of cancer at the DNA level. It detects epigenetic changes and is performed on the residual tissue from previous negative biopsies (up to 30 months old). It helps to distinguish patients who have a true-negative biopsy from those who may have occult cancer (Figure 1). The test helps find men who may benefit from an mpMRI or another biopsy and early detection.
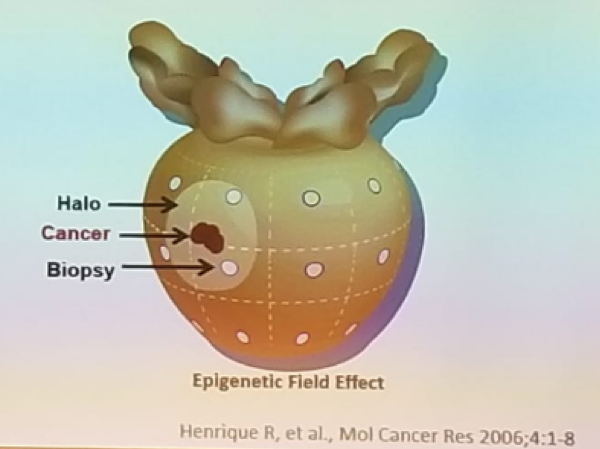
Figure 1 – The concept of ConfirmMDx test:
The next test discussed is the OncotypeDX which helps in risk stratification and monitoring of men on active surveillance. It also guides adjuvant or salvage therapy after radical prostatectomy. It incorporates multiple biologic pathways predictive of prostate cancer aggressiveness. The combination of multiple pathways is more predictive than any single pathway.
Prolaris was the next test discussed. This is based on 31 gene cell cycle progression (CCP) signature, normalized to 15 housekeeper genes. The test is performed on biopsy tissue (formalin fixed) and this test has a large role in the improved stratification of disease risk. This test has been validated in studies with more than 1300 patients.
The next discussed is the DECIPHER prostate cancer classifier, which is especially useful in the late stages of the disease, in the adjuvant and salvage therapy. This is a genomics signature test, representing multiple biological pathways involved in aggressive prostate cancer. It analyzes the expression of 22 biomarkers, and reclassifies 80% of patients, reflecting the biological heterogeneity of high-risk prostate cancer patients. It categorizes patients into low, average and high-risk disease. It has been shown to be an independent prognostic marker in predicting disease-specific survival, biochemical recurrence, and metastasis after radical prostatectomy. It is mainly indicated for patients with adverse pathology after radical prostatectomy, and it gives you the absolute risk of metastases five years following surgery.
Dr. Tilki summarized her talk, stating that biomarkers can improve prostate cancer risk assessment, reduce overtreatment, and enable more selective treatment of high-risk patients by adding genetic information to standard clinical variables. The optimal way to use biomarkers in daily practice and combine them with mpMRI is still unclear. Finally, it is unknown if treatment selection based on biomarkers influences progression-free survival, overall survival or quality of life.
Presented by: Derya Tilki, MD, Martini-Klinic, Hamburg, Germany
References:
1. Elkhoury F. AUA 2018, abstract PD23-01
2. Hubner N et al. AUA may 2017
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre Twitter: @GoldbergHanan at the 38th Congress of the Society of International Urology - October 4- 7, 2018 - Seoul, South Korea