Dr. Averch began by emphasizing that many different groups are assessing how we are providing care and what outcomes we are achieving, including the federal government, insurers, hospitals, industry, and patients.
While the importance of quality monitoring is somewhat self-evident, more practically, it is important as it contributes to payment models, contributes to regionalization, is monitored by the Joint Commission, and contributes to national rankings that patients may use when choosing care.
As of a recent AUA census, 56% of urologists participate in quality measurement. Among these, more than one-fifth say that doing so has not improved the quality of their practice, more than one-quarter say they are unsure of changes or benefits, and the remainder noted benefits in terms of financial incentives, performance assessment, or patient care workflow.
The timeline of quality measurement, in the United States, begins with the Institute of Medicine’s publication of “To err is human”. Many of the subsequent changes were then legislatively enacted.
The most recent of these, MACRA, has as its primary goal to eliminate the sustained growth rate. This program is divided into MIPs and advanced APMs. Most urologists are predominately in MIPs, which are less structured than advanced APMs, though the overall goal is for all clinicians to migrate into APMs.

The Merit-based Incentive Payment System (MIPS) incentivizes and penalizes physicians based on relevant metrics, with the four components being meaningful use of electronic health records, quality reporting, resource utilization (cost), and clinical practice improvement activities. Over time, the percentage weight assigned to each component is changing with decreasing importance of quality and the increasing importance of costs. However, for the individual clinician, improvement activities may be most controllable.
There are many ways for urologists to report their data including the use of claims data, registries such as AQUA, the electronic health record, the CMS web interface, or consumer assessments.
Dr. Averch emphasized that this is a zero-sum game – for each dollar paid out as an incentive, a dollar in penalty must be withheld. Notably, payment incentive/penalty is based on metrics from 2 years prior.
Dr. Averch then discussed Quality Process Program Measures, previously known as Core Measure and Clinical Process Measures. From a conceptual perspective, the measures are based on the Donabedian Framework considering structures, processes, and outcomes of care. At CMS, all measures are categorized within six measure domains.
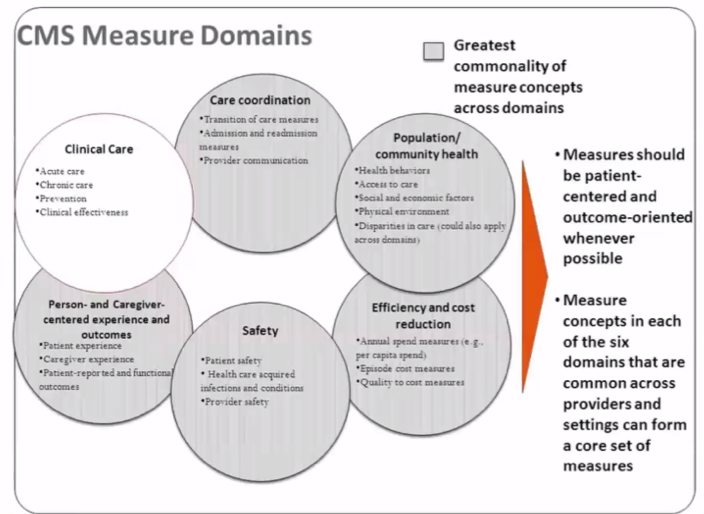
In urology, there are 28 such measures including both processes of care and outcomes. All measures have a title, definition, historical measure, a type, and the relevant domain. This is important as at least one reported domain must be an outcome measure.
Beyond these CMS-mandated activities, there are other, local quality improvement activities for which there may be incentives within the institution. At the hospital level, there are many groups and companies who perform measurement and assessment of both institution and individual level performance, including Press Gainey, NCR, and others.
Further, at the hospital level, there are many metrics for which hospitals may be penalized for poor performance. Dr. Averach emphasized that documentation is critical in the assessment of many of these metrics – where issues are either present prior to our intervention or an expected outcome of intervention may be attributable as adverse events if not appropriately noted. Further, for hospitals, he noted that 30-day readmission rates are an important metric.
He further noted that all outcomes are attributable to the “doctor”, while impacted by all members of the care team including trainees, PAs, NPs, and medical students.
Further, much of these data are publicly available, both at the hospital and physician level, through Medicare.gov.
In concluding, he emphasized that quality measurement is here to stay and it is important for each of us to understand our data.
Presented by: Timothy D. Averch, MD, Clinical Professor and Chief, Division of Urology, Palmetto Health Medical Group, Columbia, South Carolina
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center, @WallisCJD on Twitter during the 85th Annual Southeastern Section of the American Urological Association, April 23-24, 2021