The three most common standard imaging methods for detecting prostate cancer metastasis include a bone scan, computed tomography (CT), and magnetic resonance imaging (MRI). However, bone scans are time-consuming (3-4 hours) and expensive ($600-$1000), CT scans have high radiation levels and are expensive ($300-$1500), and MRIs are minimally better than CT at nodal imaging and are also expensive ($500-$2500). Dr. Morgan notes that it is important to avoid imaging in low-risk prostate cancer given the potentially harmful radiation exposure, incidental findings that require painful and risky follow-up procedures (ie. bone biopsies) and blocking access to imaging resources for other patients with the associated unnecessary increases in healthcare costs.
Being from Michigan, Dr. Morgan is part of the statewide MUSIC collaborative, which has developed imaging appropriateness criteria for newly diagnosed prostate cancer. These criteria are as follows:

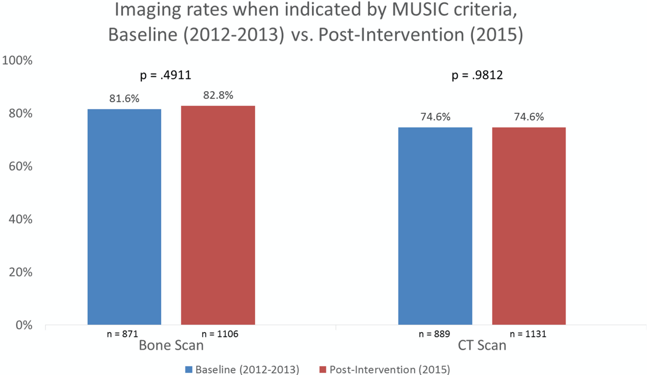
Based on the MUSIC criteria, specifically for bone scans, only 20.7% of patients would be scanned, 17.0% of scanned patients would be positive, only 0.8% of patients would have missed metastatic detection, and 38% of negative scans would be avoided. With regards to CT scans, only 22.6% of patients would be scanned, 14% of scanned patients would be positive, only 0.4% of patients would have missed metastatic detection, and 44% of negative scans would be avoided. Based on data from the MUSIC collaborative, Hurley and colleagues enrolled 10,554 newly diagnosed prostate cancer patients from January 1, 2012 through December 31, 2013 (baseline rates of imaging) and January 1, 2015, through December 31, 2015 (after employment of MUSIC imaging criteria).1 Of these patients 7,442 (79%) and 7,312 (78%) met the MUSIC criteria to avoid bone scan and CT imaging, respectively. After the multidimensional interventions to deploy the new criteria were undertaken in 2014, the use of bone scan imaging when not indicated decreased from 11.0% at baseline to 6.5% after interventions (p <0.0001). Furthermore, the use of CT imaging when not indicated decreased from 14.7% at baseline to 7.7% after interventions (p <0.0001).
The main limitations of conventional imaging are the low sensitivity and specificity. Thus, there is a need for new imaging modalities, which include whole-body MRI and PET/CT, which may include F-18 sodium fluoride, C-11 choline/acetate, F-18 fluorocholine, synthetic amino acid PET radionuclides (fluciclovine), and PSMA targeting. PET/CT as an imaging biomarker combines molecular/metabolic and anatomic imaging, providing a quantitative description of findings. 18F-fluciclovine is a synthetic amino acid analog of leucine, a marker of protein synthesis, with minimal urine excretion that has increased uptake into prostate cancer cells due to increased metabolism. Prostate specific membrane antigen (PSMA) is a 3-part membrane protein expressed in prostate cells:

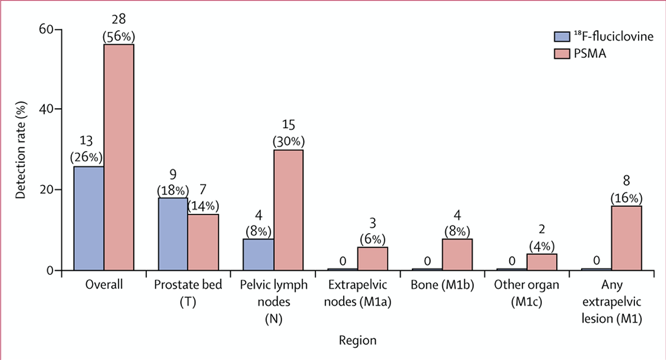
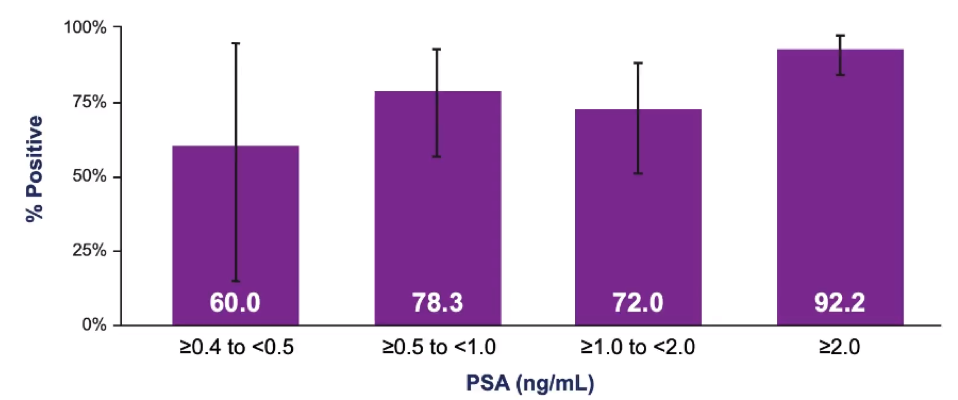
Small molecules are able to target PSMA (not antibodies), are able to penetrate solid tumors, and are rapidly cleared from the blood. Eiber et al.2 evaluated 68Ga-PSMA-11 ligand PET/CT among 248 patients with biochemical recurrence after radical prostatectomy and found detection rates were 96.8%, 93.0%, 72.7%, and 57.9% for PSA levels of ≥2, 1 to <2, 0.5 to <1, and 0.2 to <0.5 ng/mL, respectively. PSMA has also recently been compared directly to fluciclovine in patients with early biochemical recurrence after prostatectomy in a prospective, single-centre, single-arm, comparative trial.3 In this trial of 50 patients receiving both imaging modalities, detection rates were significantly lower with 18F-fluciclovine PET-CT (13 [26%; 95% CI 15-40] of 50) than with PSMA PET-CT (28 [56%; 95% CI 41-70] of 50), with an OR of 4.8 (95% CI 1.6-19.2; p=0.0026) at the patient level. In a subgroup analysis of the pelvic nodal region, disease was detected in 4 (8%; 95% CI 2-19) patients with 18F-fluciclovine compared to 15 (30%; 95% CI 18-45) patients with PSMA PET-CT (OR 12.0, 95% CI 1.8-513.0, p=0.0034):
The recently published CONDOR trial assessed the novel 18F-DCFPyL tracer in 208 patients with biochemically recurrent disease.4 Patients with positive 18F-DCFPyL-PET/CT scans based on local interpretation were scheduled for follow-up within 60 days to verify suspected lesion(s) using a composite standard of truth. As their primary outcome of interest, the authors assessed the correct localization rate, defined as the percentage of patients with a 1:1 correspondence between at least one lesion identified by 18F-DCFPyL-PET/CT and the composite standard of truth: pathology, correlative imaging, or PSA response. Using the defined primary outcome of correct localization rate, CONDOR demonstrated that 18F-DCFPyL-PET/CT correctly localized lesions in 84.8-87.0% of cases against the composite standard of truth.
Using local radiographic assessment, PSMA-avid lesion(s) were found in 142 of 208 patients (69.3%). As a result, more than two-thirds of patients enrolled in this study (131 of 205, 63.9%) had a change in intended management following 18F-DCFPyL-PET/CT.
The proPSMA study assessed the role of PSMA-PET/CT in the initial staging of high-risk patients and was published in 2020 in the Lancet.5 Following enrollment, patients were randomly assigned in a 1:1 ratio to either conventional imaging performed using bone scan and CT or PSMA-PET/CT. The primary study outcome was the accuracy of first-line diagnostic imaging for the identification of either pelvic nodal or distant metastatic disease. There were 302 patients enrolled of whom 300 received assigned first-line imaging. In the primary outcome assessment, PSMA-PET/CT had a 27% absolute greater AUC for accuracy compared to conventional imaging (95% CI 23-31): 92% (95% CI 88-95%) vs 65% (95% CI 60-69%). Additionally, conventional imaging had both a lower sensitivity (38% vs 85%) and also a lower specificity (91% vs 98%).
Dr. Morgan notes that the more we use molecular imaging, the higher number of oligometastatic cases we will see, thus resulting in a stage migration:
The challenge will lie in how we treat these patients, likely combining prostate directed therapy, systemic therapy, and metastasis-directed therapy.
Dr. Morgan concluded his presentation with the following take-home messages:
- CT and Tc-99m bone scan imaging is on the verge of being obsolete
- PSMA PET is superior to the existing radiotracers for the detection of metastatic prostate cancer
- The use of PSMA PET will have a large impact on clinical care
- 68Ga-PSMA-11 is currently approved at UCSF and UCLA and DCFPyL is expected later this year
Presented by: Todd Morgan, MD, Professor, Urology, University of Michigan, Ann Arbor, MI
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md during the 85th Annual Southeastern Section of the American Urological Association, April 23-24, 2021
References:
- Hurley P, Dhir A, Gao Y, et al. A Statewide Intervention Improves Appropriate Imaging in Localized Prostate Cancer. J Urol. 2017 May;197(5):1222-1228.
- Eiber M, Maurer T, Souvatzoglou M, et al. Evaluation of hybrid 68Ga-PSMA ligand PET/CT in 248 patients with biochemical recurrence after radical prostatectomy. J Nucl Med. 2015 May;56(5):668-674.
- Calais J, Ceci F, Eiber M, et al. 18F-fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: A prospective, single-centre, single-arm, comparative trial. Lancet Oncol 2019 Sep;20(9):1286-1294.
- Morris MJ, Rowe SP, Gorin MA, et al. Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study. Clin Cancer Res. 2021 Feb 23 [Epub ahead of print].
- Hofman MS, Lawrentschuk N, Francis, RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomized, multicentre study. Lancet 2020 Apr 11;395(10231):1208-1216.