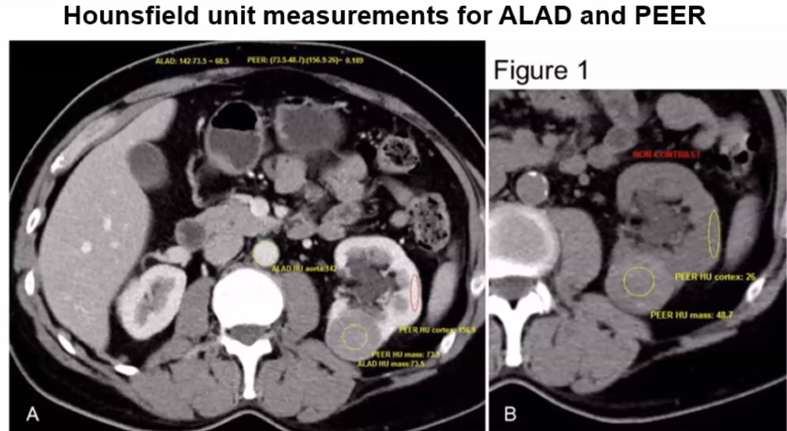
The cohort was comprised of 119 patients who presented with a renal mass and underwent partial or radical nephrectomy performed by a single surgeon. Patients were only included if a preoperative contrast-enhanced CT scan was available for evaluation and the resected renal mass was pathologically confirmed for chromophobe RCC (n=29), oncocytoma (n=62), or clear cell RCC (n=28). To calculate the ALAD value, Hounsfield units of the aorta and renal mass were measured on the same plane of contrast-enhanced CT. ALAD is expressed by the following equation: ALAD = HUaorta – HUmass. To calculate PEER, Hounsfield units of the lesion and renal cortex adjacent to the lesion were measured on contrast-enhanced CT and non-contrast CT. PEER is expressed as (HUcontrast tumor - HUnon-contrast tumor) : (HUcontrast cortex - HUnon-contrast cortex).
Values were retrospectively measured from contrast-enhanced CT by a single reviewer.
The ALAD median was 27.6 for oncocytoma, 68.5 for chromophobe RCC, and 55.4 for clear cell RCC. A significant difference between ALAD values of oncocytoma and chromophobe RCC was observed in the nephrographic (area under the ROC curve [AUC] 0.92) and excretory phases (AUC 0.95) but was less successful using contrast-enhanced CT scans lacking distinct phases (AUC 0.58). The PEER median was 0.74 for oncocytoma and 0.37 for chromophobe RCC. PEER values significantly differed while comparing oncocytoma and chromophobe RCC in the nephrographic (AUC 0.93) and excretory phases (AUC 0.96) and was also successful on contrast-enhanced CT scans lacking distinct phases (AUC 0.90, p=0.002). When differentiating between chromophobe RCC and oncocytoma among all CT phases, PEER (AUC 0.93) significantly outperformed ALAD (AUC 0.80) (p=0.008). Secondarily, all masses with a central scar on CT were pathologically confirmed to be an oncocytoma (p<0.001), and including the mass size did not improve the ability of ALAD or PEER to differentiate between benign or malignant lesions.
Dr. Lomax concluded his presentation with the following take-home messages:
- This data suggests that the ability of ALAD to differentiate between malignant and benign lesions is dependent on CT contrast phase, whereas the ability of PEER to differentiate between chromophobe RCC and oncocytoma is consistent across CT contrast phases
- ALAD and PEER values can significantly differentiate between chromophobe RCC and oncocytoma on preoperative contrast-enhanced CT
Presented by: Steven Lomax, MD, urologist, Mayo Clinic, Jacksonville, Florida
Co-Authors: Amanda Kahn1, Colleen Ball2, David Thiel1
1Mayo Clinic, Department of Urology, Jacksonville, FL, 2Mayo Clinic, Division of Biomedical Statistics and Informatics, Jacksonville, FL
References:
1. Khan AE, Lomax SJ, Bajalia EM, et al. Utility of the Aortic-Lesion-Attenuation-Difference (ALAD) and Peak Early-Phase Enhancement Ratio (PEER) to differentiate benign from malignant renal masses. Can J Urol. 2020 Aug;27(4):10278-10284.