(UroToday.com) In the United States, cancers of the kidney and renal pelvis comprise the 6th most common newly diagnosed tumors in men and 10th most common in women, with new diagnoses exceeding 65,000 patients annually. For patients with large or locally advanced renal tumors, radical nephrectomy (RN) is a commonly used treatment approach. Perioperative mortality ranges from 0.5-3.6%. Mortality risk scores have been derived and validate for patients undergoing radical cystectomy while no such predictor is available for patient-level risk prediction for patients undergoing radical nephrectomy. Below is the prior work among patients undergoing radical cystectomy.
In Best of Podium presentation at this year’s Southeast Section of the American Urologic Association Virtual Annual Meeting, Dr. Marley and colleagues assessed whether this score could be used for patients undergoing radical nephrectomy.
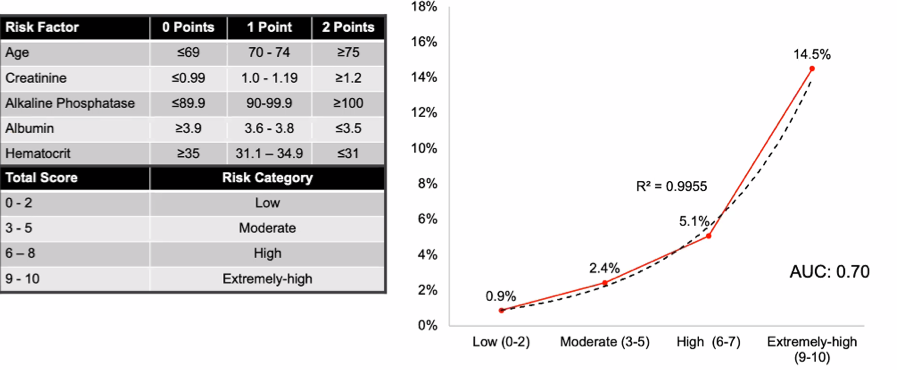
To do so, the authors utilized the National Surgical Quality Improvement Program to identify 16,617 patients who underwent RN for renal or upper urinary tract malignancy between 2013-2017. They then used backward stepwise binary logistic regression to identify independent risk factors for 30-day mortality following surgery. The authors examined the previously developed mortality risk score for each patient (Figure panel A). The authors then assessed the discriminatory ability of the risk score to predict 30-day mortality using a receiver operating characteristic (ROC) curve.
Among the 16,617 patients undergoing radical nephrectomy, 9,345 had complete data for analysis. 6,112 (65%) patients underwent laparoscopic or robotic-assisted surgery. Among included patients, the mean age was 64±12 years, the mean body mass index was 30.3±7.0 kg/m2, and most patients were male (n=5950, 64%).
The postoperative 30-day mortality rate was 1.2% (n=116). Older age, elevated creatinine, lower albumin and hematocrit, congestive heart failure, exertional dyspnea, >10% weight loss, disseminated cancer, and open operative technique were associated with increased rates of mortality.
Following radical nephrectomy, 30-day mortality increased with increasing risk categories among the mortality risk score (p<0.00001). The relative risk of 30-day mortality significantly increased among each escalating risk category (compared to low risk): moderate risk = 4.8 (95% CI, 2.5-9.1, p<0.00001), high risk = 16.8 (9.0-31.5, p<0.00001), and extremely high risk = 36.8 (13.4-101.2, p<0.00001). 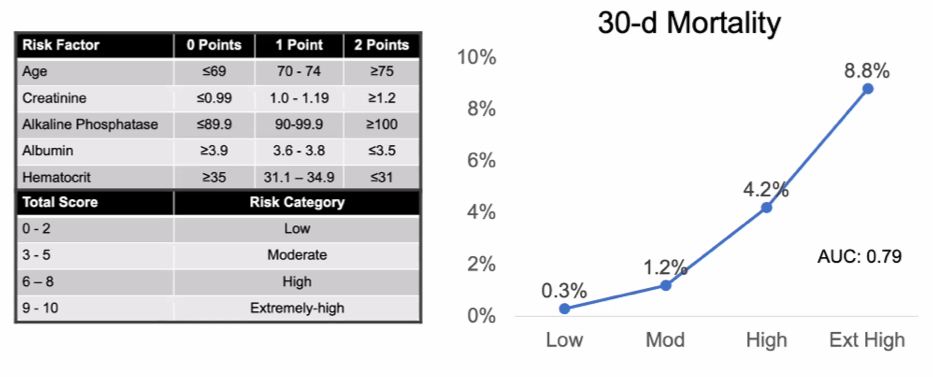
Assessing the discriminatory ability of the risk score to predict 30-day mortality using a receiver operating characteristic (ROC) curve, the authors found that the area under the curve (AUC) was 0.794 (95% CI, 0.755-0.832), which was significantly better than chance alone (p<0.00001). The discriminatory ability of the risk score was similar for patients undergoing minimally invasive RN (AUC, 0.785; 95% CI, 0.722-0.849; p<0.00001) and open RN (AUC, 0.781; 95% CI, 0.730-0.832; p<0.00001).
In conclusion, the authors demonstrated that a previously developed and validated mortality risk score in radical cystectomy may be used to predict mortality following radical nephrectomy.
Presented by: Kristen Marley, MD, Urology Resident at The University of Tennessee Health Science Center
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center during the 85th Annual Southeastern Section of the American Urological Association, April 23-24, 2021