(UroToday.com) The 2026 SESAUA annual meeting featured a kidney cancer session and a presentation by Dr. Maxwell Sandberg discussing a study from the Intercontinental Collaboration of RCC assessing the impact of cytoreductive nephrectomy for RCC with tumor thrombus. Cytoreductive nephrectomy with tumor thrombectomy is a treatment option for patients with metastatic RCC with tumor thrombus. However, there is a paucity of research examining metastatic RCC with tumor thrombus patients at diagnosis, especially looking at the role of cytoreductive nephrectomy with tumor thrombectomy. As such, the purpose of this study, presented at the SESAUA 2026 annual meeting, was to report survival outcomes on metastatic RCC with tumor thrombus patients who underwent cytoreductive nephrectomy with tumor thrombectomy.
This was a retrospective study performed using data from the Intercontinental Collaboration on Renal Cell Carcinoma (ICORCC) database. ICORCC is a multi-institutional collaboration that focuses specifically on RCC tumor thrombus and includes institutions from North America, Central and South America, Spain, and South Korea. Patients required an imaging confirmed diagnosis of metastatic RCC with tumor thrombus, with either a CT and/or MRI scan, and had to undergo cytoreductive nephrectomy with tumor thrombectomy. Tumor thrombus was graded using the Mayo Clinic Classification system. Metastatic locations were qualified as either lung, bone, brain, liver, retroperitoneum, adrenal, para-aortic nodes, or “other nodes.” Overall survival and cancer specific survival were calculated, and progression free survival was tracked and defined as either imaging confirmed evidence of recurrence at the nephrectomy bed and/or new evidence of metastatic disease aside from that on preoperative imaging. Cox proportional hazards regression was used to assess the significance of demographic variables, treatment characteristics, and location of metastases on survival time to event measures within five years of surgery.
A total of 131 patients with metastatic RCC with tumor thrombus underwent cytoreductive nephrectomy with tumor thrombectomy between 1999 and 2024. The median number of metastatic sites at the time of cytoreductive nephrectomy with tumor thrombectomy was 1 (IQR 1-2). Fifty-six (44%) patients had a level I tumor thrombus, 31 (24%) had a level II tumor thrombus, 20 (16%) had a level III tumor thrombus, and 20 (16%) had a level IV tumor thrombus. Median five-year overall survival was 1.7 years (95% CI 0.6-4.9), median five-year cancer specific survival was 2.2 years (95% CI 0.7-5.3), and median five-year progression free survival was 1.1 years (95% CI 0.3-2.9) after cytoreductive nephrectomy with tumor thrombectomy:
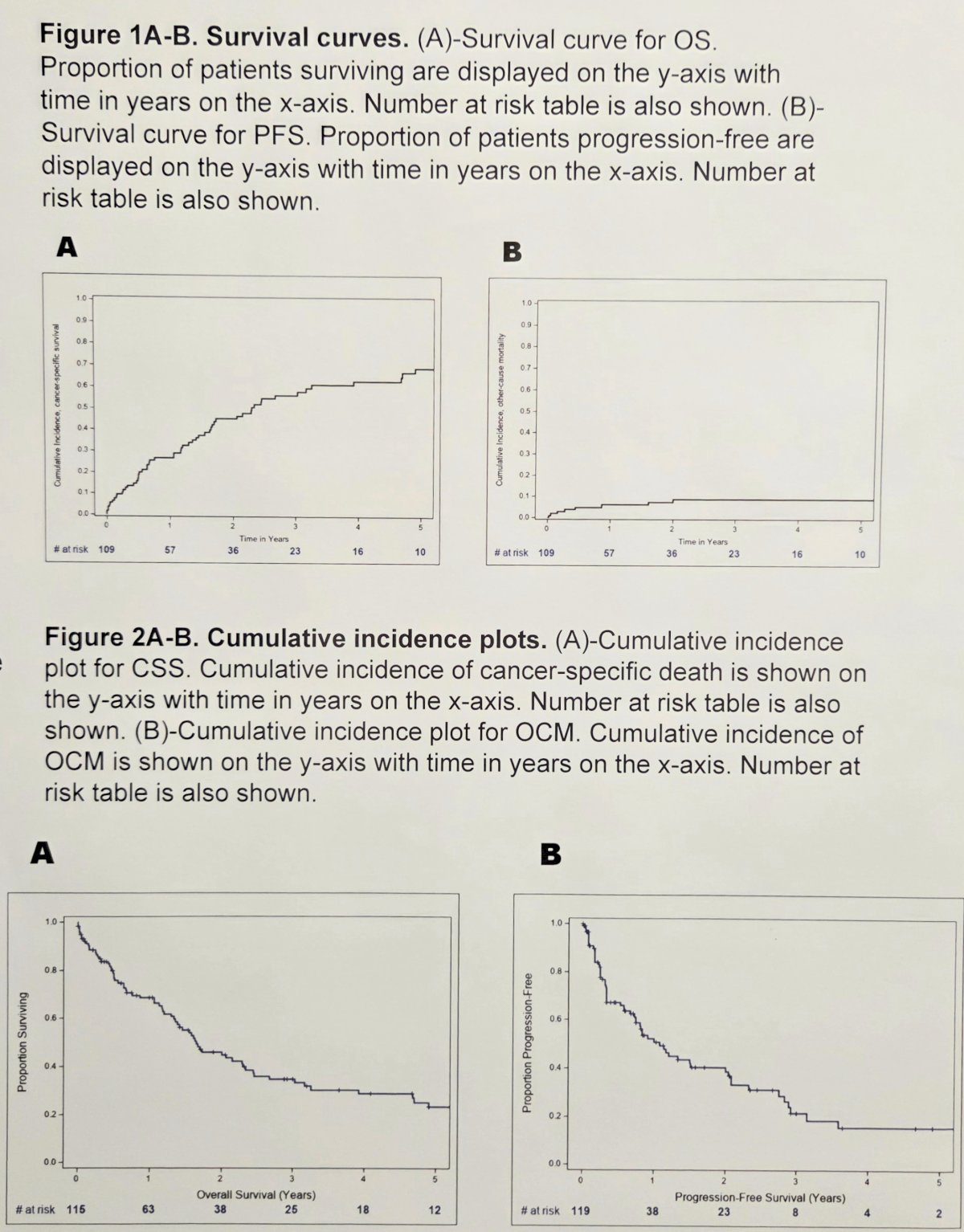
Patients with systemic symptoms at diagnosis (HR 2.2, p = 0.0056), larger tumor size (for each 1cm: HR 1.14, p = 0.0013), and adrenal metastases (HR 5.3, p = 0.0005) had a greater hazard of death. On competing risks regression models for cancer specific survival, the presence of brain metastases conferred a hazard ratio of 3.4 (p = 0.024) for cancer specific death.
Dr. Sandberg concluded his presentation discussing a study from the Intercontinental Collaboration of RCC assessing the impact of cytoreductive nephrectomy for RCC with tumor thrombus with the following take-home points:
- Overall survival and cancer specific survival are poor after cytoreductive nephrectomy with tumor thrombectomy
- Systemic symptoms at diagnosis, large preoperative tumor size, and adrenal metastases predicted a greater hazard of death post-operatively
- Progression free survival was poor, with no predictable co-variables identified
- Brain metastases predicted a greater likelihood of cancer specific death
- These findings call for prospective validation to identify those patients most likely to benefit from cytoreductive nephrectomy with tumor thrombectomy
Presented by: Maxwell Sandberg, MD, Wake Forest Baptist Medical Center, Winston-Salem, NC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Southeastern Section of the American Urological Association (SESAUA) Annual Meeting, San Juan, PR, Wed, Mar 18 – Sat, Mar 21, 2026.